Robyn Higgins and I wrote a chapter about cultural safety in the arts in an exciting new book about community engaged arts practice The Relationship is the Project edited by Jade Lillie with Kate Larsen, Cara Kirkwood and Jax Jacki Brown.
It is exciting to be in such a fabulous line up with folks like Genevieve Grieves about working in First Nations contexts; Caroline Bowditch on access and disability; Dianne Jones, Odette Kelada and Lilly Brown on racial literacy; and other contributors including: Esther Anatolitis, Adolfo Aranjuez, Paschal Berry, Lenine Bourke, Tania Cañas, Rosie Dennis, Alia Gabres, Eleanor Jackson, Samuel Kanaan-Oringo, Fotis Kapetopoulos, Kate Larsen, Lia Pa’apa’a, Anna Reece, Daniel Santangeli, and Jade Lillie.
Here’s a tiny excerpt from our chapter to whet your appetite.
Why do we need cultural safety?
Australia is a white settler colony in which British invasion and colonisation have institutionalised whiteness. Like other sectors, this history is strongly reflected in the arts, including the ways our practitioners, organisations and institutions develop and deliver projects in collaboration with artists and communities.
Arts organisations often prioritise and centre whiteness. For people and communities who are not white, these organisations may not be seen as appropriate, accessible or acceptable, which can prevent participation and engagement.
Since I wrote this post the chapter has been edited and reprinted twice:
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2020/01/RITP.jpg960720ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2020-01-24 12:25:322020-01-24 12:25:32Cultural safety in the arts
I wrote a piece for the Australian College of Nursing’s (ACN) quarterly publication. Cite as: DeSouza, R. (Summer 2019/20 edition). The potential and pitfalls of AI. The Hive (Australian College of Nursing), 28(10-11).
Many thanks to Gemma Lea Saravanos for the photo.
The biggest opportunity that Artificial Intelligence (AI) presents is not the elimination of errors or the streamlining of workload, but paradoxically the return to caring in health. In eliminating the need for health professionals to be brilliant, as machines will be better at diagnosis and other aspects of care, the need for emotional intelligence will become more pressing.
In his book Deep medicine, he recounts how he grew up with a chronic condition, osteochondritis dissecans which was disabling. At 62, a knee replacement surgery went badly wrong, followed by an intense physical protocol which led to devastating pain and distress leaving him screaming in agony. Topol tried everything to get relief and his orthopaedic surgeon advised him to take antidepressants. Luckily his wife found a book called Arthrofibrosis, which explained why he was suffering a rare complication of inflammation affecting 2-3% of people after a knee replacement. His surgeon could only offer him future surgery, but a physiotherapist with experience of working with people with osteochondritis dissecans (OCD), offered a gentler approach that helped him recover. AI could have helped him by creating a bespoke protocol which took into account his history which the doctor did not. The problems of health care won’t be fixed by technology, but the paradox is that AI could help animate care, in the case of the robotic health professionals he had to deal with in the quest of recovery.
The three D’s
Nursing practice is being radically transformed by new ways of knowing including Artificial Intelligence (AI), algorithms, big data, genomics and more, bringing moral and clinical implications (Peirce et al., 2019). On one hand, these developments have massive benefits for people, but they also raise important ethical questions for nurses whose remit is to care for patients (Peirce et al., 2019). In order for nurses to align themselves to their values and remain patient centred they need to understand the implications of what Topol calls the three D’s: the digitisation of human beings through technological developments such as sensors and sequencing are digitally transforming health care; the democratising of medicine as patient’s knowledge of themselves becomes their possession rather than that of the health system and lastly, deep learning, which involves pattern recognition and machine learning.
Data is fundamental to AI
The massive amounts of data being collected -from apps, wearable devices, medical grade devices, electronic health records, high resolution images and whole genome sequences- allows for increased capability in computing to enable the effective analysis and interpretation of such data, and therefore, making predictions.
Artificial Intelligence (AI) includes a range of technologies which can work on data to make predictions out of patterns. Alan Turing, who is thought to be the founding father of AI, defined it as the science of making computers intelligent; in health AI uses algorithms and software to help computers analyse data (Loh, 2018).
Applications of AI Data are transforming health in two key ways:
Assisting with enhancing patient care – from improving decision making and making diagnosis more effective and accurate to recommending treatment. Systemising onerous tasks to make systems more effective for health care professionals and administrators.
Applications are emerging including automated diagnosis from medical imaging (Liu et al., 2019), surgical robots (Hodson, 2019), trying to predict intensive care unit (ICU) mortality and 30-day psychiatric readmission from unstructured clinical and psychiatric notes (Chen, Szolovits, & Ghassemi, 2019), skin cancer diagnosis; heart rhythm abnormalities, interpreting medical scans and pathology slides, diagnosing diseases, and predicting suicide using pattern recognition, having been trained on millions of examples.
These systems overcome the disadvantages of being a human for example being tired or distracted. And from a knowledge translation point of view, rather than waiting for knowledge to trickle down from research into practice over decades, steps could be automated and more personalised (Chen et al., 2019).
AI can also be used to better serve populations who are marginalised. For example, we know that not everyone is included in the gold standard of evidence: randomised trials. This means that they are not representative of entire populations, so therapies and treatments may not be tailored to marginalised populations (Chen et al., 2019; Perez, 2019).
Potential for algorithmic bias in health However, large annotated data sets on which machine learning tasks are trained aren’t necessarily inclusive. For example image classification through deep neural networks may be trained on ImageNet,which has 14 million labelled images. Natural language processing requires that algorithms are trained on data sets scraped from websites that are usually annotated by graduate students or via crowdsourcing which then unintentionally produce data which embeds gender, ethnic and cultural biases. (Zou & Schiebinger, 2018).
This is because the workforce that designs, codes, engineers and programs AI may not be from diverse backgrounds and the future workforce are a concern also as gender and ethnic minorities are poorly represented in schools or Universities (Dillon & Collett, 2019).
Zou & Schiebinger (2018) cite three examples of where AI applications systematically discriminate against specific populations- the gender biases in the ways google translate converts Spanish language items into English; software in Nikon cameras that alert people when their subject is blinking, identify “Asians “as always blinking and word embedding, an algorithm for processing and analysing natural-language data, identifies European American names as “pleasant” and African American ones as “unpleasant”.
Other similar contexts include crime and policing technologies and financial sector technologies (Eubanks, 2018; Noble, 2018; O’Neill, 2016). Also see (Buolamwini & Gebru, 2018). But, how does one counter these biases? As Kate Crawford (2016) points out “Regardless, algorithmic flaws aren’t easily discoverable: How would a woman know to apply for a job she never saw advertised? How might a black community learn that it were being overpoliced by software?”.
Biased decision-making in a systematic way might happen with individual clinicians but they also rely on clinical judgement, reflection, past experience and evidence.
Digital literacies for an ageing workforce We have a crisis in healthcare, and in nursing. Our technocratic business models with changes from above are contributing to “callous indifference” (Francis, 2013). Calls to reinstate empathy and compassion in health care, and ensure care is patient-centered, reflect that these features are absent from care.
In the meantime, we have had Royal Commissions into aged care, disability and mental health. For AI to be useful, it’s important that nurses understand how technology is going to change practice. Nurses already experience high demands and complexity in their work, so technological innovations that are driven from the top down risk alienating them and further burning them out (Jedwab, et al. 2019). We are also going to have to develop new models of care that are patient centred and codesigning these innovations with diverse populations is going to become increasingly important.
References Buolamwini, J., & Gebru, T. (2018). Gender Shades: Intersectional Accuracy Disparities in Commercial Gender Classification. In S. A. Friedler & C. Wilson (Eds.), Proceedings of the 1st Conference on Fairness, Accountability and Transparency (pp. 77–91). Retrieved from http://proceedings.mlr.press/v81/buolamwini18a.html Chen, I. Y., Szolovits, P., & Ghassemi, M. (2019). Can AI Help Reduce Disparities in General Medical and Mental Health Care? AMA Journal of Ethics, 21(2), E167–E179. https://doi.org/10.1001/amajethics.2019.167 Crawford, K. (2016, June 25). OpinionArtificial Intelligence’s White Guy Problem. The New York Times. Retrieved from https://www.nytimes.com/2016/06/26/opinion/sunday/artificial-intelligences-white-guy-problem.html Dillon, S., & Collett, C. (2019). AI and Gender: Four Proposals for Future Research. Retrieved from https://www.repository.cam.ac.uk/handle/1810/294360 Eubanks, V. (2018). Automating Inequality: How High-Tech Tools Profile, Police, and Punish the Poor. Retrieved from https://market.android.com/details?id=book-pn4pDwAAQBAJ Hodson, R. (2019). Digital health. Nature, 573(7775), S97. https://doi.org/10.1038/d41586-019-02869-x Jedwab, R. M., Chalmers, C., Dobroff, N., & Redley, B. (2019). Measuring nursing benefits of an electronic medical record system: A scoping review. Collegian , 26(5), 562–582. https://doi.org/10.1016/j.colegn.2019.01.003 Liu, X., Faes, L., Kale, A. U., Wagner, S. K., Fu, D. J., Bruynseels, A., … Denniston, A. K. (2019). A comparison of deep learning performance against health-care professionals in detecting diseases from medical imaging: a systematic review and meta-analysis. The Lancet Digital Health, 1(6), e271–e297. https://doi.org/10.1016/S2589-7500(19)30123-2 Loh, E. (2018). Medicine and the rise of the robots: a qualitative review of recent advances of artificial intelligence in health. BMJ Leader, 2(2), 59–63. https://doi.org/10.1136/leader-2018-000071 Noble, S. U. (2018). Algorithms of Oppression: How Search Engines Reinforce Racism. Retrieved from https://market.android.com/details?id=book–ThDDwAAQBAJ O’Neill, C. (2016). Weapons of math destruction: How big data increases inequality and threatens democracy. Nueva York, NY: Crown Publishing Group. Peirce, A. G., Elie, S., George, A., Gold, M., O’Hara, K., & Rose-Facey, W. (2019). Knowledge development, technology and questions of nursing ethics. Nursing Ethics, 969733019840752. https://doi.org/10.1177/0969733019840752 Perez, C. C. (2019). Invisible Women: Exposing Data Bias in a World Designed for Men. Retrieved from https://play.google.com/store/books/details?id=MKZYDwAAQBAJ Zou, J., & Schiebinger, L. (2018). AI can be sexist and racist — it’s time to make it fair. Nature, 559(7714), 324–326. https://doi.org/10.1038/d41586-018-05707-8
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2020/01/Hivecover-768x1024-1.jpeg1024768ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2020-01-14 14:46:062020-01-14 14:46:06The potential and pitfalls of AI.
Cultural safety in health is the radical idea that people who use health services should be treated with competence, care and respect, so that their dignity and sovereignty are maintained, and not compromised by the system of health care. Both an ethical framework for negotiating relationship and an outcome of care, cultural safety rests on transforming power relations and disrupting universal factory models of care premised on an ideal implicit service user, who is typically able bodied, straight, cis gendered, white and middle class. Cultural safety provides a counter to the reductionism and individualism of episodic care in medicine, to demand that the health of recipients of care whether as individuals, families or communities is holistic and seen in the context of historical and geographical determinants.
There’s an extensive bibliography on the genesis of cultural safety, but briefly it’s a concept developed in Aotearoa, New Zealand by Māori nurses that’s travelled to other white settler nations like Canada, and contexts including the arts. It is a really exciting time for the concept of cultural safety in Australia as it gains momentum among Indigenous health advocates but more broadly in health contexts, challenging inter-changeably used terms like cultural awareness and cultural competence. Mark Lock has beautifully outlined developments in his article on How to Embed Cultural Safety in Healthcare Governance – Better Boards. These developments include:
The Medical Board of Australia, public consultation on a draft revised code of conduct including a revised section on culturally safe and sensitive practice with Aboriginal and Torres Strait Islander peoples (June 2018).
The Nursing and Midwifery Board of Australia–care is ‘culturally safe and respectful’ (2018).
The Australian Health Practitioner Regulation Authority (AHPRA) committing to embedding cultural safety in the 15 national health practitioner boards (July 2018).
The Council of Australian Governments’ (COAG) Health Council public consultation on reforms of the Health Practitioner Regulation National Law (July 2018).
The National Safety and Quality Health Service Standards now contain six new actions for implementation in 2019, where achieving these actions means ‘provide culturally safe care’ for Aboriginal and Torres Strait Islander peoples (2019).
$350,000 for Australian-first online cultural safety training course for nurses and midwives delivering care to Aboriginal and Torres Strait Islander peoples (January 2019).
Recently, The Australian Health Practitioner Regulation Agency (AHPRA) asked for feedback on the definition of ‘cultural safety’ both from the public and specifically from Aboriginal and Torres Strait Islander individuals and organisations. The public consultation which closes next week (May 24th 2019) is led by the National Registration and Accreditation Scheme’s Aboriginal and Torres Strait Islander Health Strategy Group (Strategy Group) and the National Health Leadership Forum (NHLF), with the aim being to develop a definition that can be embedded more broadly. This is the proposed definition they want feedback on
‘Cultural safety is the individual and institutional knowledge, skills, attitudes and competencies needed to deliver optimal health care for Aboriginal and Torres Strait slander Peoples as determined by Aboriginal and Torres Strait Islander individuals, families and communities.
I really recommend reading the incisive and comprehensive critique of AHPRA’s definition of cultural safety in Croakey. Dr Leonie Cox (Queensland University of Technology) and Associate Professor Odette Best (University of Southern Queensland) argue that changing the definition from Māori scholar Dr Irihapeti Merenia Ramsden’s critical work replaces a political imperative with an individualised, ethnographic and idealised version which places the burden for health system transformation to the consumer in the guise of partnership. Cox and Best (2019) observe:
Let us be clear, cultural safety is about the cultures of systems, professions and practitioners. It is about an ongoing individual and organisational self-reflective exercise. It addresses the impact that mainstream cultures, ways of doing business and social positions have on practice and on health outcomes for service users.
I am pleased to have been involved in related initiatives happening in Victoria. In November 2018 I was invited to speak at the Victorian Clinical Council meeting, an independent group, which provides leadership and independent advice to the Department of Health and Human Services and Safer Care Victoria (SCV) on how to make the health system safer. The council had chosen the theme of diversity and cultural safety. In my presentation, I provided an overview of cultural safety. I also suggested a shift in focus from the language of diversity, to one that addresses power and privilege using critical tools like intersectionality and cultural safety. I shared the five facts about cultural safety and encouraged the council to ask disruptive questions and explore alternative ideas and perspectives. You can read more hereCommunique meeting 4 2018 (PDF, 130.27 KB). You can see the recommendations which will be presented to SCV and the department Secretary to endorse and action.
In April 2019, I was invited to be a keynote at Safer Care Victoria’s first Partnering in healthcare forum. The theme ‘Together is better’ is a reflection of a genuine commitment to ensure consumers are at the centre of care. Three hundred attendees attended the sold out event over two days to focus on how to best respond to the needs and expectations of consumers and deliver care that is person centred, equitable and caring. What impressed me ever so much is that Safer Care Victoria worked hard to support consumers to take part and over a hundred participants identified as having a consumer background. SCV have also developed a Partnering in healthcare framework. I have had a long interest in power relations in health and in examining how concepts like choice, partnership and empowerment can transfer responsibility to service users but without the access to infrastructure, resources and support. I loved David Gilbert’s presentation. David is a Consumer Director in the National Health Service, UK and he spoke about the role of consumers and patients and how the notion of ‘patient leadership’ in the UK is transforming roles, opportunities, and models of patient partnership. In a fabulous article in the BMJ, David says:
Meanwhile, I watch the failure of the engagement industry—reliant on child-parent feedback mechanisms and adolescent-parent institutional arrangements that pit representatives against professionals (or co-opt them) in tedious sub-sub-committees. And yields… not much to be honest. Everywhere I look, power is neutralised and buffered. We are patted on the head, told to play with broken toys rather than join in with the big boys. The passion and wisdom gained through suffering and resilience is not valued. This is a caricature, but I believe it largely represents recent reality.
I really appreciated what David said about what we call people who try to change the system rather than healing in peace. occupy what do we call idiots like me who, instead of just wanting to heal in peace, return to the NHS in a different guise?
There were so many other highlights at the Partnering Forum which gave me great heart. One of the standouts (and I know I should mention every single one) was by Clinical Lead and Facilitator for the Rounds, Associate Professor Leeroy William, Chief Experience Officer Anne Marie Hadley and Anjali Dhulia from the Schwartz Round team who provide palliative care at Monash Health. This team were highly commended in the Safer Care Victoria compassionate care award category for the ‘Rounds’ which are a structured forum for all clinical and non-clinical staff. It provides a safe and nurturing space for people to regularly come together to talk about the emotional and psychological aspects of working in health care. The idea comes from work at the Schwartz Centre for Compassionate Care in Boston. What I loved about it, is the recognition of trauma and compassion fatigue for people who work in health care which includes staff like cleaners or kitchen staff who do not get seen as part of the health care team, but often have very intimate conversations and connections with people. I think that having the space to talk about things that matter in the factory system of health care can transform burnout, negativity and cynicism, by providing a sense of community and care and mostly reconnecting people to their purpose in working in health.
Which brings me to my own presentations at the conference. I did a keynote presentation and a workshop. Rather than attempt to summarise, I’ll leave the last words and images to the most fabulous Zahra Zainal, a Melbourne-based graphic recorder and illustrator, who has so much talent and was able to simplify and amplify my words into stunning illustrations. Please feel share to use and share with appropriate acknowledgement of Zahra and I.
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2019/05/07_EquityInclusionInHealthcare.original.1556573312-1024x576-1.jpg5761024ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2019-05-20 14:12:232019-05-20 14:12:23Cultural safety: On healing the health system through partnership
I wrote a piece for the Spring 2018 edition (Issue 23) of the Hive (the Australian College of Nursing’s quarterly publication). Cite as:DeSouza, R. (2018). Is it enough? :Why we need more than diversity in nursing. The Hive (23, 14-15). You can also download a pdf of the article for your own personal use.
Diversity is a hopeful, positive and celebratory idea, it generates more happiness than words like inequity, racism and privilege. It feels good for a large number of people precisely because it is depoliticized (Hall & Fields, 2013). It does not demand accountability. It does not demand transformational change of our minds or our environment, but requests that we continue to put up with difference or to tolerate it (Bell & Hartmann, 2007). What does it mean for our profession to be diverse? And is it enough?
Is it enough, when we have a yawning chasm of health inequity and disparity, of deaths in custody, of punitive policy aimed at Aboriginal Australians? Is it enough, in an era of devastating Islamophobia and racism enabled by nationalist right wing xenophobia? Is it enough, when politicians challenge group-based rights and argue that they undermine social cohesion and “our way of life”, maligning and scapegoating already vulnerable groups like African youth. Is it enough, when media only catapult the spectacular and exceptional into our view. Is it enough, when the entire world is condemning Australia’s abhorrent offshore policy of deterrence and detention. Yes, we need to recognise difference, but we must also understand how differences are connected to inequalities. As Mohanty observes: “diversity by passes power as well as history to suggest a harmonious and empty pluralism” (Mohanty, 2003, p. 193).
We might be ticking the diversity boxes and celebrating diversity — whether in University brochures and websites or on Harmony Day — but do our combined activities address health disparities? The problems of inequity and disparity are bigger than us but we can be accountable for the parts we play in larger political struggles. For a politics of equity, we also need to consider race, disability, ethnicity, class, gender, sexuality, and religion and integrate these into our analyses of our social world. We need to expand the frames we use to look beyond individual behaviour and to consider social and systemic issues, and call for systematic interventions to address inequity. ‘Celebrating’ cultural difference isn’t the same as action, as fighting for justice. As (Perron, 2013) notes, nurses can be both caring for individuals and advocating for the collective rights to equitable care, they aren’t mutually exclusive.
Diversity assumes that care is still a neutral technical activity
As nursing emerged from being a class of handmaidens to the medical system to the dynamic profession it is today, we have understood it to become an intellectual, cultural and contextual activity. This means it is also a political activity (De Souza, 2014). Nursing is connected to systems of power and privilege. Nurses and clients bring multiple ways of being in the world into the world of care and yet we only privilege some of these ways of being. Iris Marion Young describes oppression as being “the disadvantage and injustice some people suffer not because of a tyrannical power coerces them but because of the everyday practices of a well-intentioned liberal society…” (Young, 1990, p. 41). There continue to be clear links between institutional bias in health care systems and health disparities (Hall & Fields, 2013). Let’s ask ourselves what practices we enact every day that contribute to inequity?
Diversity maintains whiteness at its core
In diversity talk in nursing there’s an assumed white centre with difference added. White people are conceived as the hosts and people of color viewed as guests and the perspectives of Indigenous people are erased. Allen (2006, pp. 1–2) calls this the ‘white supremacy’ of nursing education: an assimilationist agenda that converts diverse groups people into a singular kind of nurse, which can then add ‘others’ into the mainstream to create a multicultural environment. But, this addition reinforces rather than displaces whiteness from the centre of structures and processes of educational or clinical institutions (p.66). It’s important that we focus on whether nurses reflect the communities that they serve. But representation in the workforce doesn’t mean that the people who are culturally different have a voice in the corridors of power. There are questions also about “who’s at the decision-making table and who’s not. And what’s on the agenda and what’s not” (Brian Raymond, 2016).
Diversity focuses on sensitivity and respect rather than on the social and historical
Race and racism are determinants of health inequities (Krieger, 2014) therefore it follows that a key area where nurses could intervene is to address discrimination. It is inadequate for us to provide individualised sensitive and respectful care while ignoring the historical and structural conditions that shape health and healthcare. As nurses, we understand more than most that life is an uneven playing field – we need to bring this knowledge to the way we work as a profession. Cultural sensitivity and awareness tend to assume that racism is “out there”, rather than something that is also enacted within healthcare systems. Our claims to colorblindness reinforce the problem, as” treating people the same” doesn’t take into account their differing needs, which is one definition of what care is.
Spotted at my local market
Creating a meaningful diverse and multicultural nursing profession
in an era where both patient populations and the nursing workforce are becoming more diverse, where are the spaces for nurses to talk about both institutional and societal racism and how they impact on care? How can nurses broaden their focus from the micro-level to see the big picture, especially when they labor in unstable and under-resourced working environments (Allan, 2017)? Nurse educators must confront our own resistance to teaching about race and racism (Bond & Others, 2017) – the recent debates about the inclusion of cultural safety into the Nursing and Midwifery Codes of Conduct reflect now far we have to go. Our curricula must more explicitly embed anticolonial and intersectional perspectives into learning experiences in order to prepare nurses for not only understanding how structural inequities affect health but also for the skills to counter them (Blanchet Garneau, Browne, & Varcoe, 2016; Thorne, 2017; Varcoe, Browne, & Cender, 2014). In Australia, the Indigenous Health Curriculum Framework developed by the Committee of Deans of Australian Medical Schools, recognised the critical need to teach students about racism. In particular, it asks us to see the connection between history and current health outcomes; to be able to identify features of overt, subtle and structural racism or discrimination and to be able to address and help resolve these occurrences.
Viewing nursing as a neutral, universal activity where appreciation, sensitivity and respect are adequate, prevents us from considering nursing as a political activity where power is at play. Conversely, embedding an understanding of the historical, structural and systemic factors that shape health, into our practice will allow us to create a meaningfully inclusive – and more caring – profession. This however, requires courage, commitment and accountability. Do we have it?
References
Allan, H. (2017). Editorial: Ethnocentrism and racism in nursing: reflections on the Brexit vote. Journal of Clinical Nursing, 26(9-10), 1149–1151.
Allen, D. G. (2006). Whiteness and difference in nursing. Nursing Philosophy: An International Journal for Healthcare Professionals, 7(2), 65–78.
Bell, J. M., & Hartmann, D. (2007). Diversity in Everyday Discourse: The Cultural Ambiguities and Consequences of “Happy Talk.” American Sociological Review, 72(6), 895–914.
Blanchet Garneau, A., Browne, A. J., & Varcoe, C. (2016). Integrating social justice in health care curriculum: Drawing on antiracist approaches toward a critical antidiscriminatory pedagogy for nursing. Sydney: International Critical Perspectives in Nursing and Healthcare. Google Scholar. Retrieved from http://sydney.edu.au/nursing/pdfs/critical-perspectives/blanchet-garneau-browne-varcoe-integrating-social-justice-2.pdf
Bond, C., & Others. (2017). Race and racism: Keynote presentation: Race is real and so is racism-making the case for teaching race in indigenous health curriculum. LIME Good Practice Case Studies Volume 4, 5.
Brian Raymond, M. P. H. (2016, August 2). How Racism Makes People Sick: A Conversation with Camara Phyllis Jones, MD, MPH, PhD | Kaiser Permanente Institute for Health Policy. Retrieved August 17, 2018, from https://www.kpihp.org/how-racism-makes-people-sick-a-conversation-with-camara-phyllis-jones-md-mph-phd/
De Souza, R. (2014). What does it mean to be political? Retrieved August 21, 2018, from http://ruthdesouza.dreamhosters.com/2014/08/03/what-does-it-mean-to-be-political/
Hall, J. M., & Fields, B. (2013). Continuing the conversation in nursing on race and racism. Nursing Outlook, 61(3), 164–173.
Krieger, N. (2014). Discrimination and health inequities. International Journal of Health Services: Planning, Administration, Evaluation, 44(4), 643–710.
Mohanty, C. T. (2003). “Under Western Eyes” Revisited: Feminist Solidarity through Anticapitalist Struggles. Signs: Journal of Women in Culture and Society, 28(2), 499–535.
Perron, A. (2013). Nursing as “disobedient” practice: care of the nurse’s self, parrhesia, and the dismantling of a baseless paradox. Nursing Philosophy: An International Journal for Healthcare Professionals, 14(3), 154–167.
Thorne, S. (2017). Isn’t it high time we talked openly about racism? Nursing Inquiry, 24(4). https://doi.org/10.1111/nin.12219
Varcoe, C., Browne, A., & Cender, L. (2014). Promoting social justice and equity by practicing nursing to address structural inequities and structural violence. Philosophies and Practices of Emancipatory Nursing: Social Justice as Praxis, Eds PN Kagan, MC Smith and PL Chinn, 266–285.
Young, I. M. (1990). Throwing Like a Girl and Other Essays in Feminist Philosophy and Social Theory. Monograph Collection (Matt – Pseudo).
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2018/11/Embracing-diversity-scaled-1.jpg22722560ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2018-11-14 20:53:132018-11-14 20:53:13We need more than diversity in nursing.
The Council of Deans of Nursing and Midwifery ANZ acknowledge Aboriginal & Torres Strait Islander people as the First Nations people of Australia. The Council supports the development and implementation of cultural safety in education programs, practice, and research activities for nurses and midwives. It also recognises that the origins and context informing the development of cultural safety arise from different historical, political, economic social and ideological positions in Australia and New Zealand and therefore this will be acknowledged separately
However, this explicitly anti-racist and equity informed strategy has not gone down well with The Nurses Professional Association of Queensland Inc (NPAQ). Run by union-buster Graeme Haycroft who calls the Codes ‘racist’, the association brands itself as a non party political alternative to existing unions. Haycroft has garnered a deluge of support (despite not being political) and claims NPAQ members were not consulted and 50 per cent of NPAQ members are opposed to the Codes. Interviewed by Sky News host Peta Credlin, supporters likeAndrew Bolt have jumped into the fray with headlines screaming: Nurses forced to announce ‘white privilege’ is new racism. The hyperbole has been astounding:
What if… they’re within seconds of dying and the nurse has to fling themselves into action but they have to stop while they just announce their white privilege?
These codes were the subject of lengthy consultations with the professions of nursing and midwifery and other stakeholders including community representatives. This review was comprehensive and evidenced-based. Our union and our national body the Australian Nursing Midwifery Federation (ANMF) were active participants in these consultations.
The codes, written by nurses and midwives for nurses and midwives, seek to ensure the individual needs and backgrounds of each patient are taken into account during treatment.
There’s no doubt cultural factors, including how a patient feels while within the health system, can impact wellbeing. For example, culture and background often determine how a patient would prefer to give birth or pass away.
Every day, nurses and midwives consider a range of complex factors, including a patient’s background and culture to determine the best treatment. These codes simply articulate what is required to support safe nursing and midwifery practice for all.
Cultural safety is creating racism, not eliminating it. It’s political correctness gone mad!
Correction: Race is a proven determinant of health. The Nursing and Midwifery Codes of Conduct acknowledge racism and attempt to reduce its impact on health.
Australia is a white settler society like the United States, Canada and New Zealand. In such settler societies, colonisation and racism have had devastating effects on Indigenous health and wellbeing. These include: the theft of land and economic resources; the deliberate marginalisation and erasure of cultural beliefs, practices and language; and the forced imposition of British models of health over systems of healing that had been in Australia for millennia.
Along with the systematic destruction of these basic tools for wellbeing, interpersonal racism has also contributed to a reduction in access to health promoting resources for Indigenous communities. Cultural safety was developed and led by Indigenous nurses in New Zealand to mitigate the harms of colonisation and improve health care quality and outcomes for Māori, and this has been extended by nurses in Australia, Canada and the US.
Evidence demonstrates that health system adaptations informed by a cultural safety approach have benefits for the broader community. For example, in New Zealand, the request by Māori to have family involved in care (whānau support) have led to a more family-oriented health care system for everyone.
Myth 2
I’m white but I’ve had a hard life, who is to say that I am privileged? Why am I being called racist for being white? That’s racist! I am a nurse, I’ve been abused, I am not privileged. I fought hard for everything I have and have achieved today.
Correction: Whiteness and white privilege refers to a system, they are not an insult.
Scholar Aileen Moreton-Robinson points out that British invasion and colonisation institutionalised whiteness into every aspect of law and policy in Australia. One of the first actions of the newly formed Australian nation state in 1901 was to pass the Immigration Restriction Act restricting the entry of non-white people.
The White Australia policy ended in 1962, when some of our lawmakers today were adults. Unsurprisingly, politicians have reflected these assumptions as they have demonised successive groups of migrants and refugees.
This culture of whiteness confers dominance and privilege to those who are located as white, but is largely invisible to them, and very visible to those who are not white. Being white in a settler colony like Australia means that you can move through daily life in a world that has been designed by people who are white for people who are white.
Even accounting for class and poverty, people who are white experience privileges that are not available to people of colour. White people can’t actually be systematically oppressed on the basis of their race by Indigenous people or people of colour, because the colonial systems of governance are still in force.
As the comedian Aamer Rahman points out, so called “reverse racism” would only exist under circumstances where white people had been intergenerationally marginalised from the social and economic resources of the nation on the basis of their race. The way Graeme Haycroft from the Nurses Professional Association of Queensland Inc attempts to create equivalence between the inconvenience of having to think differently about health with generations of dispossession is farcical and insulting.
Myth 3
Why can’t we treat everyone with respect? Dividing people into categories of oppressors and victims isn’t helpful. I respect each patient and their diversity as I respect all the nurses I work with and their cultural diversity.
Correction: No matter what individuals believe, entering the health system is not always a safe experience for cultural minorities. Providing tailored care where possible helps the health system work for everyone.
One size does not fit all. It’s not helpful to treat everybody the same or to say that one does not see colour. How one shows respect varies from one person to the next. Some things work for some people, while others don’t.
Many nurses and midwives already tailor health care to people’s bodies, genders, class and sexuality. For example, the grumpy old entitled man is a well-known “type” of patient that nurses have dealt with for generations, disrupting their own routines and responding to patient demands in order to get them to accept the care required.
Cultural safety promotes an understanding of the culture of health and asks nurses and midwives to be learn to be more responsive to the needs of the patient generally, and this only benefits patients.
Cultural safety asks caregivers to challenge biases and implicit assumptions in order to improve healthcare experiences for Aboriginal and Torres Strait Islander peoples. In the codes, cultural safety also applies to any person or group of people who may differ from the nurse/midwife due to race, disability, socioeconomic status, age, gender, sexuality, ethnicity, migrant/refugee status, religious belief or political beliefs.
In other words, where “business as usual” is designed for white people, cultural safety is for everyone.
Myth 4
Why is cultural safety being regarded in the new Codes of Conduct as equally important to the patient as clinical safety? Doesn’t that devalue clinical care?
Correction: Cultural safety enhances clinical safety.
People are more likely to use health services that are appropriate, accessible and acceptable. If people don’t use health services because they do not trust them or find them unsafe, then they are more likely to become very ill or die unnecessarily.
The health system is not accessed equally by all Australians who need it. For example, Aboriginal and Torres Strait Islander people access health services at less than half of their expected need. Safety and quality of care are also linked with culture and language. Research shows that people from minority cultural and language backgrounds are more at risk of experiencing preventable adverse events compared to white patients.
In Australia lesbian, gay, bisexual, transgender, queer, and intersex (LGBTQI) people often receive inappropriate medical care, and experience health inequities compared to the general population around drug and alcohol use; sexual health and mental health issues.
Discrimination, transphobia, homophobia and a lack of cultural safety from health professionals discourage help seeking. Having services that are welcoming and safe would facilitate equitable health outcomes for all these groups.
Myth 5
There is no objective assessment of what constitutes “cultural safety”.
Correction: Only the person and/or their family can determine whether or not care is culturally safe and respectful.
The most transformative aspect of cultural safety is a patient centered care approach, which emphasises sharing decision-making, information, power and responsibility. It asks us as clinicians to demonstrate respect for the values and beliefs of the patient and their family; advocating for flexibility in health care delivery and moving beyond paternalistic models of care.
Patient-centred care is institutionalised in the Australian Charter of Health Care Rights (ACSQHC, 2007) and the Australian Safety and Quality Framework for Health Service Standards (2017) Partnering with consumers (Standard 2).
Cultural safety challenges nurses and midwives to work in partnership with people and communities but acknowledges that the system is weighted towards the interests of those who work in the system. We think we give the same care to everyone, but everyone experiences our care differently.
Once we understand ourselves and our health system as having a culture that privileges some people over others – whether we are conscious of it or not – we can get on with the real work of implementing better healthcare experiences for Aboriginal and Torres Strait Islander peoples and other marginalised groups.
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2018/03/CulturalSafety5-1.jpg13331151ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2018-03-26 20:52:552018-03-26 20:52:55Five myths about cultural safety
]De Souza, R. (2017). I Smell You, Life Matters, Radio National, Australia. Thursday 14 September 2017.
The wonderful Masako Fukui from Life Matters interviewed me for this story about olfactory assimilation.
I am a committed foodie, ‘somebody with a strong interest in learning about and eating good food who is not directly employed in the food industry’ (Johnston & Baumann, 2010, 61) who is also interested in the politics of food. In particular, the politics of food in public spaces like public transport and hospitals.
I am interested in the ways in which admission into western medical health services requires assimilation into a distinct patient subculture. This coercive incorporation and relinquishment of clothing and belongings is accompanied by the loss of autonomy over everyday activities and routines, which is ceded to health professionals and institutional processes. From being a socially integrated member of a community, the person within the dominant mode of biomedicine is reduced to being an individual, then a physical body or parts. The person becomes an object who receives care.
Food is more than sustenance and nutrition, it has social, cultural and symbolic meanings which structure not only our daily lives, but also life transitions such as maternity. Food represents an arena where powerful values and beliefs about being a human are evident. Food practices also demarcate cultural boundaries of belonging and not belonging. Forthcoming: De Souza, R. (in press). Going Without: Migrant Mothers, Food and the Postnatal Ward in New Zealand. In F. Guignard and T. Cassidy (Eds.), Moving Meals and Migrant Mothers. Toronto: University of Toronto Press.
Fish is OK, as long as it isn’t pungent. Curry is nice, as long as the spices don’t cling to the curtains. Kimchi is healthy, as long as the fermented garlic doesn’t linger on the train.
But for the migrant who feels displaced from their homeland, foods that olfactorily offend may play an important role in reinforcing identity, Dr De Souza says.
She says cooking and eating a beautiful curry is akin to “putting lotion on the part of me that feels dislocated, lonely, and isolated”. But that same curry can reek of spices that ultimately isolate her by making her smell different, even invoking disgust.
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2016/07/IMG_4798.jpg12801280ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2017-09-14 15:44:052017-09-14 15:44:05I Smell You
Margaret Atwood’s The Handmaid’s Tale focuses on women living in a theocratic totalitarian regime in a newly created dystopian, pronatalist society called Gilead. The regime attributes declining fertility to women’s rights, same sex relationships and an environment damaged beyond repair, which it solves with the creation of a society predicated on women stratified into their biological destinies to reproduce (Handmaids) or to fulfil household obligations in the private sphere (Marthas). The women are all white, and the story is told through Offred, the plucky white narrator enslaved in a white male supremacist society, where all the people of color have been banished to ‘the colonies'(we are also left uncertain about whether this includes indigenous peoples). Margaret Attwood doesn’t need to attend to characters of color in the book because in a matter of sentences we already know that they are not included in this new world. This lets Attwood off the hook for engaging with with characters of color in the novel. However, critiques of the book from an intersectional perspective have noted that the narrative banishment comes to extrapolate white women’s experiences as representative of the experiences of all women, even though many of the exploitative and cruel mechanisms to curtail maternity and bodily autonomy used on the white women were used specifically against women of colour in actual North American history that underpins the life of the author and the novel. Or were used on enslaved Africans in the United States including public lynchings and being named after their owners.
The television version attempts to address the invisibility and exclusion of the book where people of color were banished or exterminated. People of colour are visible on screen, as loving husbands, loyal running mates, a daughter, a housekeeper. The women of color characters are dispersed through the stratified roles of Handmaids or Marthas which also assumes levels of social mobility. But these characters are merely backdrop cardboard cutouts, holograms, one-dimensional, devoid of depth in this white supremacist tale. Characters like Luke and Moira don’t get to explore their racial identities, much less how religious totalitarianism would specifically affect their racialised experiences. In ignoring racism, the show misses an opportunity to show how racism would manifest and evolve in a puritanical theocracy. In the show, The Handmaid’s Tale assumes that racism has been solved or that it is trumped by gender in the cause of preserving fertility. But there is a lost opportunity to consider ‘racist sexism’, that is how policies and practices that discriminate against women, also discriminate in different ways against racialised women. It also fails to acknowledge that America hasalways been a dystopia for people of color or that American dystopia is founded on anti-Black violence.. It appears on the surface that all subjects other than the commanders and their wives are treated in much the same way as each other. Seemingly the biblical rules of law are applied equally for transgressions. But Bastien asks:
Are white Commanders and their wives really okay with having a handmaid of color? Is there a caste system for handmaids of color in which some are considered more desirable than others? Do Commanders of color have the same privileges as their white counterparts? If Gilead is meant to imagine a possible future for America, how could deeply entrenched racial dynamics disappear?
In this color-blind, post-racial idyll, there are people of color, but they are hollow and we know nothing about them, past or present. Evan Narcisse suggests it is like the comment made when you’re a non-white person in a predominantly white institution: “When I look at you, I don’t see a marginalised/minority person, I just see a person.” Although meant kindly, in its unmarked privilege it erases the fact of your difference and what it means to inhabit your body and your life. Whiteness is still the unacknowledged default. As Stephanie Brown observes, the men in power are white, as are most of the women. It’s important though that we care about all of this in real life, not just as fiction, as Berlatsky notes:
Because fictional tyrannical dystopias are primarily envisioned as affecting white people, it can be harder to see negative policies that oppress others. At the point where the fictional metaphor matters more than the current reality, something’s gone terribly wrong.
Several critics suggest that The Handmaid’s Tale represents a failure of intersectionality. The term ‘intersectionality’ originates in African American theorising and activism, and is most commonly associated with work by Kimberle Crenshaw and Patricia Collins. It describes how systems of oppression are viewed as interlocking. Therefore, attempts to dislodge one axis of oppression will impact on another. Globally, the term intersectionality is being appropriated as a way to activate attempts to address issues of under-representation in institutions without reverting to a single focus lens on issues such as gender, race, class, or sexuality. Intersectionality provides an understanding that identities can be simultaneously privileged and marginalised, depending on social context. Consequently we are all interpellated differently by racism and sexism through a ‘matrix of domination’(Collins, 1990). For example, I can be a migrant woman of color who is marginalised through sexism and racism, but I am also privileged through class position, education, able body and heterosexuality.
Intersectionality is being introduced into diversity initiatives in Universities and is gaining momentum in the Science, Technology, Engineering, Maths and Medicine disciplines (STEMM) disciplines. Intersectionality is seen as a strategy for addressing the barriers to success and to widen and increase participation by women, working class, indigenous and ethnic minority groups, in order to leverage a diversity dividend. The use of an economic metaphor valorises innovation and economic competitiveness, rather than attempting to address a pressing social justice. Metaphors to account for inequities and the underrepresentation of groups in STEMM disciplines include the old boys club, the glass ceiling and the leaky pipeline. These metaphors also guide the strategies developed to address these failures of inclusion and their limitations. Merely creating a pipeline and applying force to propel people forward does not guarantee an increase numbers (Núñez, 2014). In the case of a pipeline, we know that it leaks at various stages and is still designed for an implicit ideal input, consequently women and ethnic minorities are more likely than white men to leak out. We also know that the leaking is progressive, so the farther along the pipeline, the fewer these groups are in number(Clark Blickenstaff*, 2005). Merely focusing on increasing or diversifying the supply hides the real issue which is at the ‘demand’ end of things, that is, the organization and the need for it to change(Riegle‐Crumb, 2009, p. 4). Similarly, the metaphor of the glass ceiling assumes the barriers facing marginalised groups are a one dimensional insurmountable barrier experienced at the ‘top’, when in fact marginalised identities experience discrimination and ‘hurdles’ throughout their careers(Husu, 2001, p. 177). Instead the analytic of intersectionality is being vaunted as an antidote to under-representation.
Diversity management is fast becoming a feature of the public image of the corporatised entrepreneurial academy. Standing in for structural or organisational change, diversity risks reproducing the issues I’ve identified in the screen version in the Handmaid’s Tale. Damon Williams suggests there are several political, social and economic imperatives for Universities to respond to diversity. In its place in the knowledge based global economy, it must respond to changing demographics and meet the need for creative and capable students and also demonstrate the viability and vibrancy of diversity. The diversity management strategies it employs range from access and equity; to creating a multicultural and inclusive campus climate; enhancing domestic and international diversity research and scholarship and preparing students for a diverse and global world (Damon Williams, p.19). However, the emphasis on diversity as a way of increasing numbers and improving Human Resources, is often not supplemented with an explicit engagement with the systems of power and inequality that structure the processes of knowledge production. Consequently, the white, elite and middle class structures and structural arrangements that reproduce inequality remain both invisible and intact (Dill & Zambrana, 2009). The neoliberal assumption of an asocial and ahistorical individualised world of meritocracy, means sometimes ignoring racism and sexism (Ong, Wright, Espinosa, & Orfield, 2011). Unmarked white, masculine values and norms instituted through colonial processes of political, cultural, and military dominance favor dominant epistemologies which claim universal truths that overlook social locations and identities (Carlone & Johnson, 2007).
The Handmaid’s Tale is being flagged as a universal wake-up call, about a white feminist dystopia. But as critics note, this ‘feminist’ rallying point ignores enduring prior calls by indigenous and women of color and is a failure of intersectionality. The assumption of a post-racial, ahistorical world limits the possibilities of imagining alternative futures for people of color, in a time of Turnbull, Trump, Macron and Trudeau. Similarly efforts in academia to engage with ‘diversity’ without attention to intersectionality and attending to systems of power and inequality, risks positioning people of color as economic resources who are mere backdrop in a white supremacist institution.
Refs
Amery, F., Bates, S., Jenkins, L., & Savigny, H. (2015). Metaphors on Women in Academia: A Review of the Literature, 2004–2013. In At the Center: Feminism, Social Science and Knowledge (pp. 245–267). emeraldinsight.com.
Archer, L., Dawson, E., DeWitt, J., Seakins, A., & Wong, B. (2015). “Science capital”: A conceptual, methodological, and empirical argument for extending bourdieusian notions of capital beyond the arts. Journal of Research in Science Teaching, 52(7), 922–948.
Ball, S. J. (2015). Accounting for a sociological life: influences and experiences on the road from welfarism to neoliberalism. British Journal of Sociology of Education, 36(6), 817–831.
Bolden, R., Gosling, J., O’Brien, A., Peters, K., Ryan, M. K., Haslam, S. A., … Winklemann, K. (2012). Academic leadership: changing conceptions, identities and experiences in UK Higher Education. Leadership Foundation for Higher Education,.
Cech, E. A., Metz, A., Smith, J. L., & deVries, K. (2017). Epistemological Dominance and Social Inequality. Science, Technology & Human Values, 0162243916687037.
Clark Blickenstaff, J. (2005). Women and science careers: leaky pipeline or gender filter? Gender and Education, 17(4), 369–386.
Collins, P. H. (1990). 2000. Black Feminist Thought: Knowledge, Consciousness, and the Politics of Empowerment.
Carlone, H. B., & Johnson, A. (2007). Understanding the science experiences of successful women of color: Science identity as an analytic lens. Journal of Research in Science Teaching, 44(8), 1187–1218.
Dill, B. T., & Zambrana, R. E. (2009). Emerging Intersections: Race, Class, and Gender in Theory, Policy, and Practice. Rutgers University Press.
Dodson, D.J. (1997). “We lived in the blank white spaces”: Rewriting the Paradigm of Denial in Atwood’s The. Utopian Studies, 8(2), 66–86.
Evans, M. (2004). Killing Thinking: Death of the University. Bloomsbury Publishing.
Eveline, J., & Booth, M. (2004). “Don’t write about it”: Writing “the other” for the ivory basement. Journal of Organizational Change Management, 17(3), 243–255.
Ferguson, H., & Wheat, K. L. (2015). Early career academic mentoring using Twitter: the case of# ECRchat. Higher Education Policy and Management. Retrieved from http://www.tandfonline.com/doi/abs/10.1080/1360080X.2014.991533
Fitzgerald, T. (2014). Advancing knowledge in higher education: Universities in turbulent times: Hershey, PA: IGI Global.
Harding, S. (1989). Taking Responsibility for Our Own Gender, Race, Class: Transforming Science and the Social Studies of Science. Rethinking Marxism, 2(3), 7–19.
Husu, L. (2001). On metaphors on the position of women in academia and science. NORA: Nordic Journal of Women’s Studies, 9(3), 172–181.
Jones, S. R. (2016). Authenticity in leadership: Intersectionality of identities. New Directions for Student Leadership, Winter 2016(152), 23–34.
Ko, L. T., Kachchaf, R. R., Ong, M., & Hodari, A. K. (2013). Narratives of the double bind: Intersectionality in life stories of women of color in physics, astrophysics and astronomy. AIP Conference Proceedings, 1513(1), 222–225.
Lynch, K. (2006). Neo-Liberalism and Marketisation: The Implications for Higher Education. European Educational Research Journal, 5(1), 1–17.
Lynch, K., Grummell, B., & Devine, D. (2012). Crafting the Elastic Self: Gendered Experiences of Senior Management. In New Managerialism in Education (pp. 134–153). Palgrave Macmillan UK.
Mignolo, W. (2000). The Many Faces of Cosmo-polis: Border Thinking and Critical Cosmopolitanism. Public Culture, 12(3), 721–748.
Miller, R. A., & Vaccaro, A. (2016). Queer Student Leaders of Color: Leadership as Authentic, Collaborative, Culturally Competent. Journal of Student Affairs Research and Practice, 53(1), 39–50.
Naidoo, R. (2003). Repositioning Higher Education as a Global Commodity: Opportunities and challenges for future sociology of education work. British Journal of Sociology of Education, 24(2), 249–259.
Núñez, A.-M. (2014). Advancing an Intersectionality Framework in Higher Education: Power and Latino Postsecondary Opportunity. In M. B. Paulsen (Ed.), Higher Education: Handbook of Theory and Research (pp. 33–92). Springer Netherlands.
Ong, M., Wright, C., Espinosa, L., & Orfield, G. (2011). Inside the Double Bind: A Synthesis of Empirical Research on Undergraduate and Graduate Women of Color in Science, Technology, Engineering, and Mathematics. Harvard Educational Review, 81(2), 172–209.
Riegle‐Crumb, C. (2009). Removing Barriers: Women in Academic Science, Technology, Engineering, and Mathematics . Edited by Jill M. Bystydzienski and Sharon R. Bird. Bloomington: Indiana University Press, 2006. Pp. 347. 75.00 (cloth); 29.95 (paper). The American Journal of Sociology, 114(4), 1231–1233.
Ruderman, M. N., & Ernst, C. (2004). Finding yourself: How social identity affects leadership. Leadership in Action, 24(3), 3–7.
Slaughter, S., & Rhoades, G. (2004). Academic Capitalism and the New Economy: Markets, State, and Higher Education. JHU Press.
Su, F., & Wood, M. (2017). Cosmopolitan Perspectives on Academic Leadership in Higher Education. (Camilla Erskine Tanya Fitzgerald, Ed.). Bloomsbury Publishing.
Williams, D. A. (2013). Strategic Diversity Leadership: Activating Change and Transformation in Higher Education. Stylus Publishing, LLC.
Winter, R. (2009). Academic manager or managed academic? Academic identity schisms in higher education. Journal of Higher Education Policy and Management, 31(2), 121–131.
Zaharia, S. E., & Gibert, E. (2005). The Entrepreneurial University in the Knowledge Society. Higher Education in Europe, 30(1), 31–40.
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2017/05/the-handmaids-tale.0.jpg533800ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2017-05-15 12:55:102017-05-15 12:55:10What can The Handmaid’s Tale teach us about intersectionality in institutional life?
I am visiting the University of Auckland as an international speaker for the Research Café on Migration & Inequality being organised by the Faculty of Science and School of Population Health. The Research Café is a project of the Engaged Social Science Research Initiative and funded by the Vice-Chancellor’s Strategic Development Fund. I’ll also be giving a public lecture on Wednesday 7th December in Room 730-268 at the School of Population Health: 11.30am -12.20pm:
“Wearables” are a growing segment within a broader class of health technologies that can support healthcare providers, patients and their families as a means of supporting clinical decision-making, promoting health promoting behaviours and producing better health literacies on both sides of the healthcare professional-consumer relationship. Mobile technologies have the potential to reduce health disparities given the growing ubiquity of smartphones as information visualisation devices, particularly when combined with real-time connections with personal sensor data. However despite the optimism with which wearable health technology has been met with, the implementation of these tools is uneven and their efficacy in terms of real-world outcomes remains unclear. Wearables have the potential to reduce the cultural cognitive load associated with health management, by allowing health data collection and visualisation to occur outside the dominant languages of representation and customised to a user experience. However, typically, “wearables” have been marketed toward and designed for consumers who are “wealthy, worried and well”. How can these technologies meet the needs of culturally diverse communities?
This presentation reports on the findings from a seminar and stakeholder consultation organised by The Centre for Culture, Ethnicity and Health, in partnership with the University of Melbourne’s Research Unit in Public Cultures and the Better Health Channel. The consultation brought together clinicians, academics, developers, community organisations, and policymakers to discuss both the broader issues that wearable technologies present for culturally and linguistically diverse (CALD) communities, as well as the more specific problems health-tracking might pose for people from diverse backgrounds. This presentation summarises the key issues raised in this consultation and proposes future areas of research on wearable health technologies and culturally and linguistically diverse (CALD) communities.
Dr. Ruth De Souza is the Stream Leader, Research Policy & Evaluation at the Centre for Culture, Ethnicity & Health in Melbourne. Ruth has worked as a nurse, therapist, educator and researcher. Ruth’s participatory research with communities is shaped by critical, feminist, and postcolonial approaches. She has combined her academic career with governance and community involvement, talking and writing in popular and scholarly venues about mental health, maternal mental health, race, ethnicity, biculturalism, multiculturalism, settlement, refugee resettlement, and cultural safety.
Contact for Information: Dr Rachel Simon Kumar r.simon-kumar@auckland.ac.nz
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2016/07/jawbone.jpg558992ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2016-12-04 19:30:202016-12-04 19:30:20Six questions for culture in the age of consumer health technologies: Public lecture
I have had several tooth adventures. The time I rather enthusiastically pushed my middle sister on her bicycle and she fell over the handlebars breaking a tooth (or was that the time I helped her break her collar-bone?). My own dental fluorosis (a developmental disturbance of enamel that results from ingesting high amounts of fluoride during tooth mineralization) and my mother’s sobering experience of periodontal disease. Not to mention my parents’ adventures in dental tourism, but I’ll save those for another time.
Apart from the personal injunction to clean and floss my teeth, I didn’t think too much about oral health as a mental health clinician until I’d left clinical practice for education, when I found myself at AUT University in a faculty committed to inter-professional education and practice, where “current or future health professionals to learn with, from, and about one another in order to improve collaboration and the quality of care.”
We had learned about oral health as undergraduate nurses, particularly about post-operative oral health care and oral health for older people. But even when working in acute mental health units, community mental health and maternity, I hate to admit, oral health wasn’t on my mind. Unsurprisingly, evidence shows that even though oral health is a major determinant of general health, self esteem and quality of life, it often has a low priority in the context of mental illness (Matevosyan 2010).
As the programme leader of health promotion at AUT, a colleague in the oral health team asked me to talk to her students about the connections between mental health and oral health and that’s when my journey really began. I also had the pleasure of getting my teeth cleaned and checked at the on site Akoranga Integrated Health at AUT whose services were provided by final year and post graduate health science students under close supervision of a qualified clinical team.
It made me think about how oral health care is performed in a highly sensual area of the body. I learned that oral tissues develop by week 7 and the foetus can be seen sucking their thumb. It made me think about how suckling and maternal bonding are critical after birth. It made me think about how we use our mouths to express ourselves and to smile or show anger or shyness, literally 65% of of our communication. It made me think about kissing in intimate relationships and therefore also about how it’s not at all surprising that our mouths also represent vulnerability and that people might consequently suffer from fear and anxiety around oral health treatment. This can range from slight feelings of unease during routine procedures to feelings of extreme anxiety long before treatment is happening (odontophobia). Reportedly, 5-20% of the adult population reports fear or anxiety of oral health care, which can lead to avoidance of dental treatment and common triggers can include local anaesthetic injection and the dental drill.
Poor oral health has a detrimental effect on one’s quality of life. Loss of teeth impairs eating, leading to reduced nutritional status and diet-related ill health. A quarter of Australians report that they avoid eating some foods as a consequence of the pain and discomfort caused by their poor dental health. Nearly one-third found it uncomfortable to eat in general. Oral disease creates pain, suffering, disfigurement and disability. Almost one-quarter of Australian adults report feeling self-conscious or embarrassed because of oral health problems, impacting on enjoyment of life, impairing social life or leading to isolation with compromised interpersonal relationships
People with severe mental illness are more likely to require oral health care and have 2.7 times the general population’s likelihood of losing all their teeth (Kisely 2016). Women with mental illness have a higher DMFT index (the mean number of decayed, missing, and filled teeth) (Matevosyan 2010). In particular, oral hygiene may be compromised. For people who experience mood disorders, depressive phases can leave person feeling worthless, sad and lacking in energy, where maintaining a healthy diet and oral hygiene become a low priority. The increased energy of manic episodes can mean energy is diffused, concentration difficulties and poor judgement. People who experience mental ill health and who self-medicate with recreational drugs and alcohol can further exacerbate poor oral health. Furthermore, drug side effects can compromise good oral health by increasing plaque and calculus formation (Slack-Smith et al. 2016). It is important for mental health support staff to provide information regarding oral health, in particular education about xerostomic (dry mouth) effects of drug treatment and strategies for managing these effects including maintaining oral hygiene, offering artificial saliva products, mouthwashes and topical fluoride applications.
There are organisational and professional barriers to better oral health in mental health care. Mental health nurses do not routinely assess oral health or hygiene and lack oral health knowledge or have comprehensive protocols to follow. As Slack-Smith et al. (2016) note there are few structural and systemic supports in care environments with multiple competing demands. Research shows that dentists are more likely to extract teeth than carry out complex preventative or restorative care in this population. Mental health clinicians are reluctant to discuss oral health and in turn oral health practitioners are not always prepared for providing care to patients with mental health disorders.
Which brings me to the topic of this blog post. Until the 17th century, medical care and dental care were integrated, however, dentistry emerged as a distinct discipline, separate from doctors, alchemists and barbers who had had teeth removal in their scope of practice (Kisely 2016).
Cox, S.; A Country Toothdrawer; Wellcome Library; http://www.artuk.org/artworks/a-country-toothdrawer-125814
I spent the weekend at the Putting the Mouth Back into the Body conference, an innovative, multidisciplinary health conference hosted by North Richmond Community Health. It got me thinking about the place of the mouth in the body and developed my learning further. The scientific method and the mechanistic model of the body central to the western biomedical conception of the body, have led us to see the body in parts which can be attended to separately from each other. And yet we know what affects one part of the body affects other parts. There’ll be an official outcomes report produced from the conference, but I thought I’d capture some of my own reflections and learning in this blog post.
Equity and the social determinants of dental disease
Tooth decay is Australia’s most prevalent health problem with edentulism (loss of all natural teeth) the third-most prevalent health problem. Gum disease is the fifth-most prevalent health problem. Tooth decay is five times more prevalent than asthma in children. Oral conditions including tooth decay, gum disease, oral cancer and oral trauma create a ‘burden’ due to their direct effect on people’s quality of life and the indirect impact on the economy. There are also significant financial and public health implications of poor oral health and hygiene. Hon. Mary-Anne Thomas MP, Parliamentary Secretary for Health and Parliamentary Secretary for Carers spoke about the impact of oral health on employment. She reinforced research findings which show that people with straight teeth as 45 per cent more likely to get a job than those with crooked teeth, when competing with someone with a similar skill set and experience. People with straight teeth were seen as 58 per cent more likely to be successful and 58 per cent more likely to be wealthy. Dental health is excluded from the Australian Government’s health scheme Medicare, which means that there is significant suffering by those who cannot afford the cost of private dental care for example low-income and marginalised groups. Dental care only constitutes 6% of national health spending and comprehensive reform could be effected with the addition of less than 2 percentage points to this says a Brotherhood of St Lawrence report (End the decay: the cost of poor dental health and what should be done about it by Bronwyn Richardson and Jeff Richardson (2011)). The socially
disadvantaged also experience more inequalities in Early Childhood Caries (ECC) rates. Research has also shown that children from refugee families have poorer oral health than the wider population. A study by my colleagues at North Richmond Community Health and University of Melbourne found that low dental service use by migrant preschool children. The study recommended that health services consider organizational cultural competence, outreach and increased engagement with the migrant community (Christian, Young et al., 2015).
The interactions between oral health and general health
Professor Joerg Eberhard spoke about the interactions between oral and general health through the lifespan. His talk also demonstrated the importance of oral hygiene, not only to prevent cavities and gum disease but impact on pregnancy, diabetes and cardiovascular health. 50 to 70 per cent of the population have gingivitis and severe gum disease (periodontitis) which develop in response to bacterial accumulation have adverse effects for general health. He showed participants the interactions of oral health and general health with a focus on diabetes mellitus, cardiovascular disease and neurodegenerative diseases. Most strikingly, Eberhard’s research published in The International Journal of Cardiology in 2014, showed periodontitis could undermine the major benefits of physical activity. If you are interested in the link between oral health and non-communicable diseases, this Sydney Morning Herald article provides a great summary.
Key points:
What effects the body also affects the mouth, in fact this is bidirectional.
Early experiences impact lifelong health eg sugar preference, early cavities, diet.
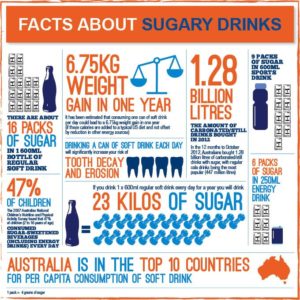
Sugar is a significant culprit
I learned a lot about sugar from Jane Martin the Exective Manager of the Obesity Policy Coalition and Clinical Associate Professor Matthew Hopcraft an Australian dentist, public health academic and television cook. 52% of Australians exceed the WHO recommendations for sugar intake, and half of our free sugars come from beverages. Sugar intake profoundly impacts cavities and our contemporary modes of industrial food production are to blame. We also need to challenge the subtle marketing of energy dense nutrient poor products eg the ubiquity of fizzy drink vending machines. To that end both Universities in the United States and health services worldwide (see NHS England) are taking the initiative to phase out the sale and promotion of sugary drinks at their sites. At the University of Sydney a group of students, researchers and academics are taking this step through the Sydney University Healthy Beverage Initiative. Check out this fabulous social marketing campaign with indigenous communities in Australia by Rethink Sugary Drink. Sugar-free Smiles advocate for public health policies and regulatory initiatives to reduce sugar consumption and improve the oral health of all Australians. There’s also the Sugar by half campaign.
Key points:
We need to think about what we are eating.
Oral health promotion and oral health literacy are important.
We need to think about the addition of sugar in foods that are ostensibly good for us (cereal and yoghurt for breakfast for example).
The case for working collaboratively: The example of pharmacists
Dr Meng-Wong Taing (Wong) from the University of Queensland persuasively argued how other professionals can have a major role in promoting both oral health and helping to lower the risk of suffering other serious conditions, such as diabetes or cardiovascular disease. Wong cited recent research findings describing the role of Australian community pharmacists in oral healthcare that show 93 per cent of all community pharmacists surveyed believed delivering oral health advice was within their roles as pharmacists. People in lower socio-economic areas often can’t afford to see a dentist and so pharmacies are the first port of call for people experiencing oral health issues. The 2013 ‘National Dental Telephone Interview Survey’, which found the overall proportion of people aged five and over who avoided or delayed visiting a dentist due to cost was 31.7 per cent, ranging from 10.7 per cent for children aged five-14 to 44.9 per cent for people aged 25-44.
IPC occurs when “multiple health workers from different professional backgrounds provide comprehensive services by working with patients, their families, carers, and communities to deliver the highest quality of care across settings” (WHO 2010, p. 13).
Key points:
How do we get oral health in health professional curricula? Particularly given the emphasis on the technocratic and acute at the expense of health promotion and public health.
How can we focus on oral health from a broader social determinants perspective?
Let’s improve access to services and oral health outcomes.
Let’s develop inter-professional approaches to undergraduate education.
Let’s develop collaborative approaches and avoiding the ‘siloing’ of oral health.
Let’s encouraging partnerships between oral health professionals and other health professionals, community groups and advocacy groups.
Perhaps the best news of the two days for me is that milk, cheese and yoghurt and presumably paneer, contain calcium, casein and phosphorus that create a protective protein film over the enamel surface of the tooth thereby reducing both the risk of tooth decay and the repair of teeth after acid attacks. This information validates my enjoyment of sparkling wine (low sugar but acidic) and cheese. Cheers.
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2016/11/Barber-teeth-768x893-1.jpg893768ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2016-11-21 14:23:352016-11-21 14:23:35Mouthing off about oral health
http://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.png00ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2016-08-26 13:49:522016-08-26 13:49:52Protected: What does it mean to be Asian in the bay?







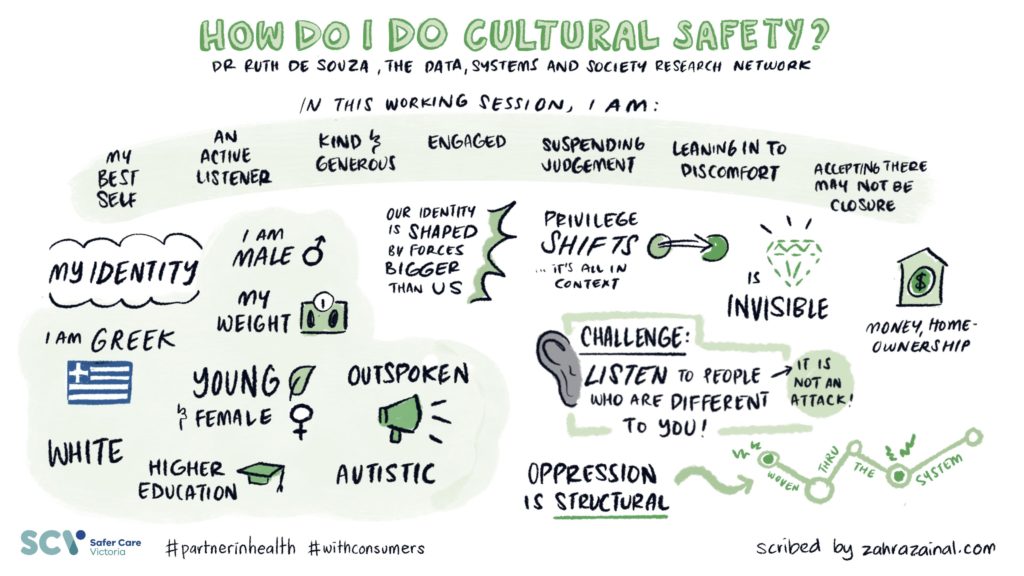
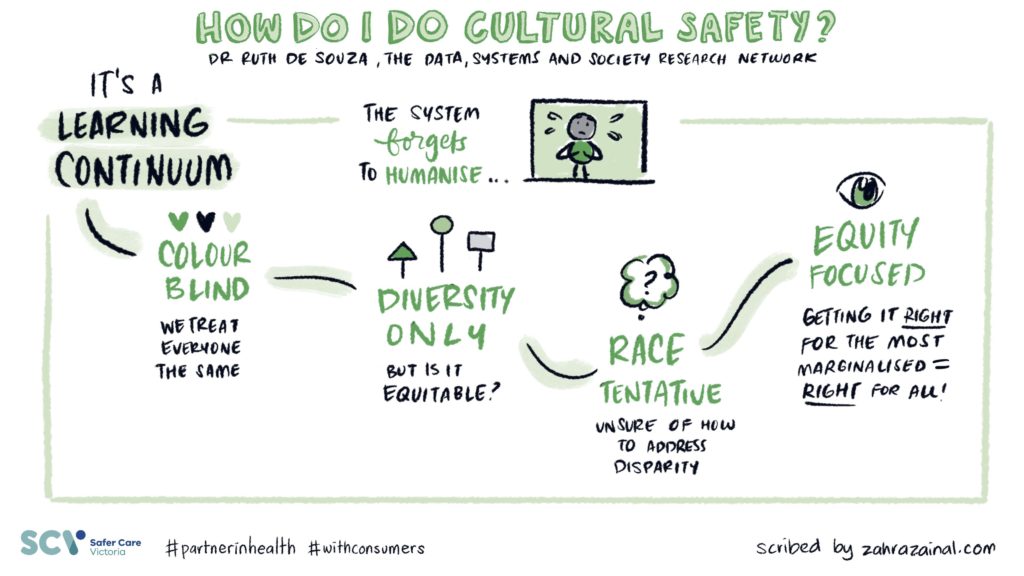










 Refs
Refs