Every week during November 2020, the indomitable Mary Freer has put together an amazing online program as part of the Compassion Revolution. It was a privilege to be in conversation with Katerina Bryant (writer and PhD student whose first book, Hysteria: A Memoir of Illness, Strength and Women’s Stories Throughout History (NewSouth) is out now; Dr Summer May Finlay (Yorta Yorta woman, public health professional and academic at the University of Wollongong) who played a pivotal part in shaping our discussion). Our session: Beyond empathy: stories that change practice was beautifully chaired by Dr Kate Bowles (Associate Dean International at the University of Wollongong Australia).
The stories of patients and those with lived experience of our health and social care systems are vital to improving the quality of our services and building our awareness and empathy. How do we challenge ourselves to go further than listening? How can we honour the stories that are so generously shared and take the lessons back to our practice?
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2020/11/IMG_7970-768x1024-1.jpg1024768ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2020-11-13 18:14:382020-11-13 18:14:38On the limits of empathy
“All bodies are not treated the same and we’re not affected by the virus in the same way… how we do healthcare actually matters… There’s some arguments that the failure to care, and poor quality [of care], are actually embedded in the structures and processes of the healthcare system.”
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2020/11/ANMFJ.jpg5661024ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2020-11-12 15:11:342020-11-12 15:11:34An interview with nurse and multi-disciplinary researcher Dr Ruth De Souza
I was invited by Hayley Singer convenor of the Environmental Arts & Humanities Network at the University of Melbourne to be a respondent to one of their seminars, exploring the COVID 19 Global Quilt Project co-instigated by artists, activists, and academics Kate Just and Tal Fitzpatrick. The @covid19quilt project started in April 2020 and the Instagram account invites people to digitally submit a textile square and a small written text about life during the COVID-19 pandemic.
The seminar series explores how environmental arts and humanities practices can help societies process social, cultural and environmental complexities by asking environmental arts, humanities scholars, artists and storytellers to reflect on ways environmental arts and humanities can provoke deep engagement, nuanced understanding, and support robust community discussion about the multiple and overlapping environmental and cultural crises of our times. Each seminar hosts an invited interdisciplinary scholar to provide a response to the primary presentation (this was me). You can listen to the webinar.
Images below are a couple of screenshots from my laptop.
On October 7th 2020 I was invited to be a keynote in The Australian Citizen Science Association (ACSA) CitSciOzOnline Early-Mid Career Researcher (EMCR) 1/2 day symposium. The aim of the symposium was to unite citizen science-aligned researchers in Australia to interrogate and explore research and practice in citizen science across the country. It featured keynotes, lightning talks, Q&A, interactive sessions, and networking opportunities, to build a community of practice in citizen science research.
My abstract Research can change the world, but how it is undertaken is not always beneficial. First Nations critiques of Western science have suggested that many aspects of research resemble colonial processes and are extractive, taking raw contextualised material from people, and making them abstract and universal for the benefit of researchers or institutions. Building on participatory action research and community-based participatory research (CBPR) methods, where researchers collaborate with community partners to investigate issues, citizen science offers a new iteration of co-producing knowledge and participating in the scientific archive outside the university. However, there are also concerns that a participatory agenda is the outcome of reduced funding, and that underfunded research institutions are using unpaid labour to produce knowledge for no cost. This presentation covers principles for working with community partners in authentic, collaborative, sensitive and culturally safe ways.
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2020/11/Citizen-science-Frog-ID.png540595ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2020-11-11 17:09:202020-11-11 17:09:20What does meaningful participation look like in Citizen Science?
“In our continued presence, blackfullas are the uncomfortable truth that this nation must reconcile itself with. We are the most courageous when it comes to conversations about race having copped the full brunt of its violence but also because we have nothing else left to lose – literally.” Chelsea Bond
Courage and racial literacy are urgently required to reconcile with uncomfortable truths in the time of COVID19 and Black Lives Matter (BLM). However, reckoning with racism is optional for some as Chelsea Bond notes, but for Aboriginal and Torres Strait Islander peoples, racism is profoundly imbricated in all the systems and structures encountered, requiring continual exhausting negotiation (see Bronwyn Fredericks, Debbie Bargallie and Bronwyn Carlson). The luxury of not having to think about racism is not available to Black people, and people of color. The aim of this blog is to facilitate discussion and share my own learning about how “we” might be more critical and reflexive in our online gatherings. I will be deliberately vague about protagonists in the spirit of using my painful experiences to educate and call in rather than shame and blame. But, yes, you know I see you!
The racialised nature of the pandemic and of police brutality, and deaths in custody, have become more perceivable for white people, some of whom are engaging in reflection and discussion on race in new ways. Gary Yonge quips that Britain has discovered racism in the same way that teenagers discover sex. Reading groups have flourished as have a proliferation of book lists. My favorite Melbourne book store Readings has a list of Books to help you understand & fight white supremacy. However, whether we can read ourselves out of racism when we did not read our way into it remains in question. The contaminated barrel needs a systemic solution not the removal of a few bad apples.
For children of empire or people of color (this term and terms like BIPOC and BAME are contentious and complicated, and are a whole other blog post), it seems an incredible opportunity to be heard and to be believed. Hanif Kureishi calls it:
our #MeToo moment, a paradigm shift, with some significant acknowledgement of how unalike the experiences of black and white people are, and of how traumatic the infliction of racism is.
Virtual meetings are par for the course, and processes that we either never imagined or thought were too difficult to replicate online have become ubiquitous. I never thought I’d do an exercise class with parents that live in another country or State, but twice a week I do Yoga for seniors on Zoom. A couple of months ago, my partner and I hosted a thirteen hour online eightieth birthday for my Mother with a hundred people in New Zealand, Canada, the US, England, Lebanon, Myanmar, India, and elsewhere. Virtual care, virtual parties, and family gatherings have seemingly seamlessly moved from real life to virtual platforms. There’s now etiquette available to help us manage conversations on a screen with multiple others. But what I am curious about is how things that were difficult face to face are possibly made even more complex and difficult in a virtual environment. Things like anti-racist work. Here I see a gap. Where’s the manual about how to create anti-oppressive spaces that do not reinscribe social relations or that center whiteness? How do people from non-dominant groups working at the interstices of social justice and pedagogical spaces look after ourselves? How can we adequately intervene in online power relations?
In my recent Zoom experiences, the invitation has been for me as a person of color (I use this term to externalise somewhat, remembering that identities are both socially constructed and individually determined) to provide counselling, forgiveness, praise or absolution. Rather like a confessional, the interlocutor wanted to recount their own experiences of witnessing racism. This is despite being the prime beneficiary of the structural arrangements in a white settler-colonial nation, and as an identity which already occupies a lot of space. This centering is an Occupational Health and Safety issue for those of us who have made it our lives work to challenge oppression wherever the miasma of institutional racism lingers. While there are a plethora of memes about the Karen and Becky’s of the world, there’s also the ‘concern troll’ who feigns concern so that they can do this very thing – distract from the process and put the focus on themselves…stalling all the work. Often, they are a loudly professed “ally” who is all about themselves and their career ambitions as the ultimate savior of, advocate for, and “scholar-activist” on behalf of “vulnerable” [black] peoples (Kati Teaiwa). Taking up space, instead of making a commitment of allyship or being an accomplice willing to undo the mechanisms that allow for the continuation of racism (Ruth Herd).
Strategies
“racism is not mine, it is yours. What you do is not called “help” when it is your mess we are cleaning.”Catherine Pugh Esq (2020)
So I have polled my Facebook pals and come up with some strategies for when as a person of color you get derailed on Zoom.
Tell the speaker to drink a cup of “shut up” juice* and move on
Ignore the speaker. Shut that down immediately and unequivocally, then avoid like COVID19 thereafter (erect walls with razor wire & border patrol much). Time spent on this BS is wasted.
Name the behaviour
“That’s an interesting anecdote. But the issues we need to focus on are …” (Tahu Kukutai).
“When you say things like X, it means other people can’t talk about Y (the reason everyone is here) and the meeting becomes about you instead. This makes people feel coopted/ exhausted/ resentful/ distracted. I can suggest somewhere you can go for a one-on-one conversation where it’s ok for it to be all about you (eg a counsellor) if you’d like?” (Alison Young).
“Thanks for being so prepared to be open and share your experiences. What we also need to work on is moving away from centering white experience. That something that we should all do in our own time. What we want to focus on here is …”
Say how you feel: “I’m tired. I deal with this every day. Please look after yourself. Bye”
Name it clearly and simply: “I feel that you take up too much space and need to leave room for others in the conversation. And I also feel like you want me to talk to you about race all the time and it’s exhausting for me.” If that doesn’t work – or you feel it’s too much to do alone – ask the moderator to help.
Use as a teachable moment
Time and energy pie-diagram. Time and energy are where power lies. Ask them about how much time and energy space they are taking. Ask them if it’s proportionate, compassionate, and aware. Ask them to ask other White people to carry some of this stuff for them, supportively, it’s their load (Karlo Mila).
Suggest a person to do the work and undertake a personal journey (in their own time. “Thank you for your contribution but this is taking a lot of important time from the class”.
Take the comment and run with it, asking a series of questions that expose the problematic effects of the comment. They will get hurt/embarrassed but the set up will mean they run to others for absolution.
Invite them to sit with their discomfort, in silence (also put this in the group agreement).
Create brave collective spaces
When acknowledging country at the start of the session, also develop group agreements that outline the purpose of the meeting.
Develop a process for people to handle their discomfort. I suggest people “lean into” their discomfort. Megan McPherson in her Acknowledgment of Country: adds “In this session, we may cover issues that may make you feel uncomfortable. I ask you to sit with this discomfort-this session is not about your discomfort, rather it is about reflecting upon your privilege and thinking about the ways you can activate your privilege and capacities, to live in Australia in better ways. I ask you this as a non-Indigenous person at XXX. It is not my Indigenous colleagues’ job to fix your discomfort about racism in Australia”.
Stay on purpose. This might mean, stressing the importance of putting off-topic issues into ‘the parking lot’ for people to pick up for themselves after the session.
Name the behaviors in the group agreement and the need for white allies to intervene and not allow it space. Revise before every meeting and participants agree before joining and revise subsequently.
Use a ‘microcosm exercise’ and ask the group to actively reflect on the how the very dynamics of the conversation in the room are a microcosm of how it works in the world, so to think about who talks, who is taking up space/time/resources, who is silent, who is doing the labor.
Invite another white person to practice solidarity, a colleague who has the competency to sit this person down and tell them that they are performing a type of aggression against you and to help them think about the impact their stories are having on people of color (Shiranthi Fonseka).
Manage questions or interactions
Provide time for people to discuss their questions and have them peer-reviewed as Eve Tuck suggests. Tuck’s twitter thread is the best thing ever written about managing Q and A sessions in ways that attend to power differentials.
Frame question and comment time in a way that asks people not to privilege their angst (Carol D’Cruz).
Have a person facilitate the Q & A (and triage the questions).
KaeLyn from Autostraddle has some great ideas including using a progressive stack to centre marginalized voices or people who are directly impacted by the issues you’re discussing. Marginalized folx could include people whose voices often don’t get heard first; people who do not share the dominant language in the room etc.
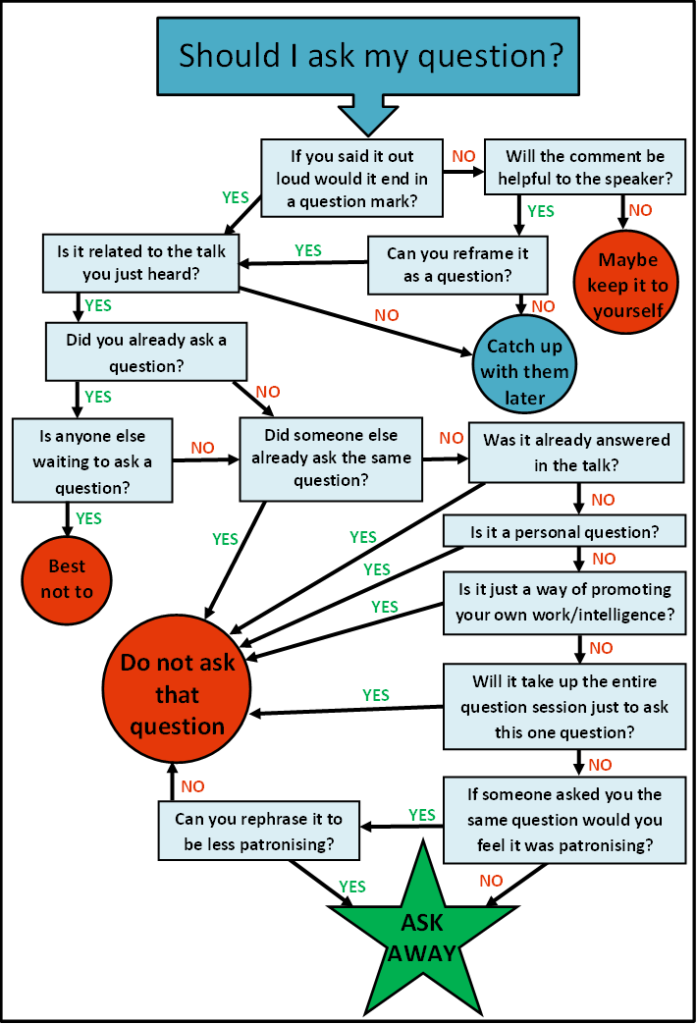
For the questioner, here is an amazing flowchart by Dani Rabaiotti, and a list of Do’s and Don’ts.
“If the first three sets of engagement with such people do not yield some movement of a shared understanding then I don’t engage. Almost always these individuals bombard you with their attention-seeking behavior at every opportunity that is made available to them. I have learned, that if I have made the initial effort and know that this person is not there to challenge themselves then holding back on giving them airtime is the best way to preserve your own energy” Tayyaba Khan.
Take care of yourself
Set parameters for yourself to maintain your own peace and energy. Also see Reni Eddo-Lodge‘s book, reference below.
Nice long hot bath & chocolates (Tee Peters).
After the event
Invite white allies to have an “after-party” where allies can support the person who feels uncomfortable (Shandra Shears Bombay).
For future events
Set boundaries for your own well-being before the event.
Create a structure where marginalized people will be given space first
Prime the moderator.
Provide the group with reading before the event.
Set boundaries about what’s appropriate and what’s not at the start.
It takes a lot of effort to make the future. One or even several demonstrations will not achieve that. The effect will be cumulative. Some things are now impossible, and other things have become possible. And so this moment of economic breakdown and capitalistic stagnation, when neo-liberalism is destroying the very ground on which it is built, is an opportunity Hanif Kureishi
Me and White Supremacy: How to Recognise Your Privilege, Combat Racism and Change the World by Layla Saad
Arao, B., & Clemens, K. (2013). From safe spaces to brave spaces: a new way to frame dialogue around diversity and social justice. In L. Landreman (Ed.), The art of effective facilitation. (pp. 135-150). Sterling, VA: Stylus
Deepest thanks to the following for their friendship and input into writing this piece.
Alex Bhathal, Sandra Shears Bombay, Esther Cowley-Malcolm, Sarah Craig, Shiranthi Fonseka, Bianca Hester, Tayyaba Khan, Tahu Kukutai, Jade Lillie, Debbi Long, Leah Manaema, Chris McBride, Rebecca McIntosh, Moata McNamara, Megan McPherson, Rebecca Monson, Laura Quin Ogle, Kat Poi, Zaky Shah, Kati Teaiwa, Nelly Thomas.
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2020/07/White-people-race.jpg540489ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2020-07-04 18:34:372020-07-04 18:34:37Virtually Racist: Anti-racist work in the time of Zoom.
Folks at Southern Crossings, a collective who aim to create space within the “Australian national imaginary and mediascape” for South Asian voices, invited Indian Australian writers to respond to the Citizen’s Amendment Act (CAA) passed on December 12, 2019 and the National Register of Citizens (NRC) in India as diasporic Indians in the context of living in Australia. These responses have been published as one statement to mirror in online form the idea of a “morcha”, a gathering of people to protest for a cause. I’ve added my thoughts below.
Australia and India are magnificent, beautiful, complicated countries that have powerfully shaped me. Goa in India is my ancestral homeland and I live as an uninvited guest on Boonwurrung country in Victoria, Australia. Although distant geographically, both countries share in the escalation of ethnonationalism and border securitisation in response to imagined threats to the culture of the nation. Australia is a British settler-colonial society that 250 years ago invaded Indigenous lands. It has relied on migration for building its nation, yet it invented and imposes the particularly cruel policy of indefinite, mandatory offshore detention. It also perpetrates colonial practices against First Nations peoples while it “celebrates” multiculturalism, and increasingly militarises its police. India suspended Article 370 of the constitution in August 2019, erasing the autonomy of Kashmir, India’s only Muslim-majority state, brutally suppressing a population of eight million people. More recently the Citizen’s Amendment Act (CAA) passed on December 12, 2019 and the National Register of Citizens (NRC) have instituted Hindu supremacy into the legislature.
The writer at the New Zealanders Against Indian Citizenship Amendment Act 2019 protest at Aotea Centre on 21 December 2019.
That two politically and militarily powerful nation states who pride themselves on secularism and the capacity to be inclusive, multicultural and multifaith are so paranoid about identity and security, and anxious about “outsiders” such as “maritime arrivals” and Muslims is breathtaking.
As we approach celebrations of Australia Day and Indian Independence day, I believe that international pressure must be put on the Indian government for its violent treatment of citizens in Kashmir; its brutality against peacefully protesting students and communities exercising their democratic right to dissent; and its discrimination against Muslims and other minority groups. I also believe that non-Indigenous Australians and the Australian government must give pause on this purportedly “national day” to consider the damage and harm to First Nations people from the violence of continuing settler colonialism, and to close the camps and resolve claims for asylum speedily in accordance with our international obligations. Here in Australia, amidst the smoke haze and a burning continent, there does not seem much to celebrate.
Photo taken by the author in the aftermath of a bushfire 2019
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2020/02/CAA.jpg1024761ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2020-02-02 12:07:162020-02-02 12:07:16What do the Citizen’s Amendment Act (CAA) and the National Register of Citizens (NRC) mean for diasporic Indians?
Robyn Higgins and I wrote a chapter about cultural safety in the arts in an exciting new book about community engaged arts practice The Relationship is the Project edited by Jade Lillie with Kate Larsen, Cara Kirkwood and Jax Jacki Brown.
It is exciting to be in such a fabulous line up with folks like Genevieve Grieves about working in First Nations contexts; Caroline Bowditch on access and disability; Dianne Jones, Odette Kelada and Lilly Brown on racial literacy; and other contributors including: Esther Anatolitis, Adolfo Aranjuez, Paschal Berry, Lenine Bourke, Tania Cañas, Rosie Dennis, Alia Gabres, Eleanor Jackson, Samuel Kanaan-Oringo, Fotis Kapetopoulos, Kate Larsen, Lia Pa’apa’a, Anna Reece, Daniel Santangeli, and Jade Lillie.
Here’s a tiny excerpt from our chapter to whet your appetite.
Why do we need cultural safety?
Australia is a white settler colony in which British invasion and colonisation have institutionalised whiteness. Like other sectors, this history is strongly reflected in the arts, including the ways our practitioners, organisations and institutions develop and deliver projects in collaboration with artists and communities.
Arts organisations often prioritise and centre whiteness. For people and communities who are not white, these organisations may not be seen as appropriate, accessible or acceptable, which can prevent participation and engagement.
Since I wrote this post the chapter has been edited and reprinted twice:
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2020/01/RITP.jpg960720ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2020-01-24 12:25:322020-01-24 12:25:32Cultural safety in the arts
I wrote a piece for the Australian College of Nursing’s (ACN) quarterly publication. Cite as: DeSouza, R. (Summer 2019/20 edition). The potential and pitfalls of AI. The Hive (Australian College of Nursing), 28(10-11).
Many thanks to Gemma Lea Saravanos for the photo.
The biggest opportunity that Artificial Intelligence (AI) presents is not the elimination of errors or the streamlining of workload, but paradoxically the return to caring in health. In eliminating the need for health professionals to be brilliant, as machines will be better at diagnosis and other aspects of care, the need for emotional intelligence will become more pressing.
In his book Deep medicine, he recounts how he grew up with a chronic condition, osteochondritis dissecans which was disabling. At 62, a knee replacement surgery went badly wrong, followed by an intense physical protocol which led to devastating pain and distress leaving him screaming in agony. Topol tried everything to get relief and his orthopaedic surgeon advised him to take antidepressants. Luckily his wife found a book called Arthrofibrosis, which explained why he was suffering a rare complication of inflammation affecting 2-3% of people after a knee replacement. His surgeon could only offer him future surgery, but a physiotherapist with experience of working with people with osteochondritis dissecans (OCD), offered a gentler approach that helped him recover. AI could have helped him by creating a bespoke protocol which took into account his history which the doctor did not. The problems of health care won’t be fixed by technology, but the paradox is that AI could help animate care, in the case of the robotic health professionals he had to deal with in the quest of recovery.
The three D’s
Nursing practice is being radically transformed by new ways of knowing including Artificial Intelligence (AI), algorithms, big data, genomics and more, bringing moral and clinical implications (Peirce et al., 2019). On one hand, these developments have massive benefits for people, but they also raise important ethical questions for nurses whose remit is to care for patients (Peirce et al., 2019). In order for nurses to align themselves to their values and remain patient centred they need to understand the implications of what Topol calls the three D’s: the digitisation of human beings through technological developments such as sensors and sequencing are digitally transforming health care; the democratising of medicine as patient’s knowledge of themselves becomes their possession rather than that of the health system and lastly, deep learning, which involves pattern recognition and machine learning.
Data is fundamental to AI
The massive amounts of data being collected -from apps, wearable devices, medical grade devices, electronic health records, high resolution images and whole genome sequences- allows for increased capability in computing to enable the effective analysis and interpretation of such data, and therefore, making predictions.
Artificial Intelligence (AI) includes a range of technologies which can work on data to make predictions out of patterns. Alan Turing, who is thought to be the founding father of AI, defined it as the science of making computers intelligent; in health AI uses algorithms and software to help computers analyse data (Loh, 2018).
Applications of AI Data are transforming health in two key ways:
Assisting with enhancing patient care – from improving decision making and making diagnosis more effective and accurate to recommending treatment. Systemising onerous tasks to make systems more effective for health care professionals and administrators.
Applications are emerging including automated diagnosis from medical imaging (Liu et al., 2019), surgical robots (Hodson, 2019), trying to predict intensive care unit (ICU) mortality and 30-day psychiatric readmission from unstructured clinical and psychiatric notes (Chen, Szolovits, & Ghassemi, 2019), skin cancer diagnosis; heart rhythm abnormalities, interpreting medical scans and pathology slides, diagnosing diseases, and predicting suicide using pattern recognition, having been trained on millions of examples.
These systems overcome the disadvantages of being a human for example being tired or distracted. And from a knowledge translation point of view, rather than waiting for knowledge to trickle down from research into practice over decades, steps could be automated and more personalised (Chen et al., 2019).
AI can also be used to better serve populations who are marginalised. For example, we know that not everyone is included in the gold standard of evidence: randomised trials. This means that they are not representative of entire populations, so therapies and treatments may not be tailored to marginalised populations (Chen et al., 2019; Perez, 2019).
Potential for algorithmic bias in health However, large annotated data sets on which machine learning tasks are trained aren’t necessarily inclusive. For example image classification through deep neural networks may be trained on ImageNet,which has 14 million labelled images. Natural language processing requires that algorithms are trained on data sets scraped from websites that are usually annotated by graduate students or via crowdsourcing which then unintentionally produce data which embeds gender, ethnic and cultural biases. (Zou & Schiebinger, 2018).
This is because the workforce that designs, codes, engineers and programs AI may not be from diverse backgrounds and the future workforce are a concern also as gender and ethnic minorities are poorly represented in schools or Universities (Dillon & Collett, 2019).
Zou & Schiebinger (2018) cite three examples of where AI applications systematically discriminate against specific populations- the gender biases in the ways google translate converts Spanish language items into English; software in Nikon cameras that alert people when their subject is blinking, identify “Asians “as always blinking and word embedding, an algorithm for processing and analysing natural-language data, identifies European American names as “pleasant” and African American ones as “unpleasant”.
Other similar contexts include crime and policing technologies and financial sector technologies (Eubanks, 2018; Noble, 2018; O’Neill, 2016). Also see (Buolamwini & Gebru, 2018). But, how does one counter these biases? As Kate Crawford (2016) points out “Regardless, algorithmic flaws aren’t easily discoverable: How would a woman know to apply for a job she never saw advertised? How might a black community learn that it were being overpoliced by software?”.
Biased decision-making in a systematic way might happen with individual clinicians but they also rely on clinical judgement, reflection, past experience and evidence.
Digital literacies for an ageing workforce We have a crisis in healthcare, and in nursing. Our technocratic business models with changes from above are contributing to “callous indifference” (Francis, 2013). Calls to reinstate empathy and compassion in health care, and ensure care is patient-centered, reflect that these features are absent from care.
In the meantime, we have had Royal Commissions into aged care, disability and mental health. For AI to be useful, it’s important that nurses understand how technology is going to change practice. Nurses already experience high demands and complexity in their work, so technological innovations that are driven from the top down risk alienating them and further burning them out (Jedwab, et al. 2019). We are also going to have to develop new models of care that are patient centred and codesigning these innovations with diverse populations is going to become increasingly important.
References Buolamwini, J., & Gebru, T. (2018). Gender Shades: Intersectional Accuracy Disparities in Commercial Gender Classification. In S. A. Friedler & C. Wilson (Eds.), Proceedings of the 1st Conference on Fairness, Accountability and Transparency (pp. 77–91). Retrieved from http://proceedings.mlr.press/v81/buolamwini18a.html Chen, I. Y., Szolovits, P., & Ghassemi, M. (2019). Can AI Help Reduce Disparities in General Medical and Mental Health Care? AMA Journal of Ethics, 21(2), E167–E179. https://doi.org/10.1001/amajethics.2019.167 Crawford, K. (2016, June 25). OpinionArtificial Intelligence’s White Guy Problem. The New York Times. Retrieved from https://www.nytimes.com/2016/06/26/opinion/sunday/artificial-intelligences-white-guy-problem.html Dillon, S., & Collett, C. (2019). AI and Gender: Four Proposals for Future Research. Retrieved from https://www.repository.cam.ac.uk/handle/1810/294360 Eubanks, V. (2018). Automating Inequality: How High-Tech Tools Profile, Police, and Punish the Poor. Retrieved from https://market.android.com/details?id=book-pn4pDwAAQBAJ Hodson, R. (2019). Digital health. Nature, 573(7775), S97. https://doi.org/10.1038/d41586-019-02869-x Jedwab, R. M., Chalmers, C., Dobroff, N., & Redley, B. (2019). Measuring nursing benefits of an electronic medical record system: A scoping review. Collegian , 26(5), 562–582. https://doi.org/10.1016/j.colegn.2019.01.003 Liu, X., Faes, L., Kale, A. U., Wagner, S. K., Fu, D. J., Bruynseels, A., … Denniston, A. K. (2019). A comparison of deep learning performance against health-care professionals in detecting diseases from medical imaging: a systematic review and meta-analysis. The Lancet Digital Health, 1(6), e271–e297. https://doi.org/10.1016/S2589-7500(19)30123-2 Loh, E. (2018). Medicine and the rise of the robots: a qualitative review of recent advances of artificial intelligence in health. BMJ Leader, 2(2), 59–63. https://doi.org/10.1136/leader-2018-000071 Noble, S. U. (2018). Algorithms of Oppression: How Search Engines Reinforce Racism. Retrieved from https://market.android.com/details?id=book–ThDDwAAQBAJ O’Neill, C. (2016). Weapons of math destruction: How big data increases inequality and threatens democracy. Nueva York, NY: Crown Publishing Group. Peirce, A. G., Elie, S., George, A., Gold, M., O’Hara, K., & Rose-Facey, W. (2019). Knowledge development, technology and questions of nursing ethics. Nursing Ethics, 969733019840752. https://doi.org/10.1177/0969733019840752 Perez, C. C. (2019). Invisible Women: Exposing Data Bias in a World Designed for Men. Retrieved from https://play.google.com/store/books/details?id=MKZYDwAAQBAJ Zou, J., & Schiebinger, L. (2018). AI can be sexist and racist — it’s time to make it fair. Nature, 559(7714), 324–326. https://doi.org/10.1038/d41586-018-05707-8
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2020/01/Hivecover-768x1024-1.jpeg1024768ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2020-01-14 14:46:062020-01-14 14:46:06The potential and pitfalls of AI.
Cultural safety in health is the radical idea that people who use health services should be treated with competence, care and respect, so that their dignity and sovereignty are maintained, and not compromised by the system of health care. Both an ethical framework for negotiating relationship and an outcome of care, cultural safety rests on transforming power relations and disrupting universal factory models of care premised on an ideal implicit service user, who is typically able bodied, straight, cis gendered, white and middle class. Cultural safety provides a counter to the reductionism and individualism of episodic care in medicine, to demand that the health of recipients of care whether as individuals, families or communities is holistic and seen in the context of historical and geographical determinants.
There’s an extensive bibliography on the genesis of cultural safety, but briefly it’s a concept developed in Aotearoa, New Zealand by Māori nurses that’s travelled to other white settler nations like Canada, and contexts including the arts. It is a really exciting time for the concept of cultural safety in Australia as it gains momentum among Indigenous health advocates but more broadly in health contexts, challenging inter-changeably used terms like cultural awareness and cultural competence. Mark Lock has beautifully outlined developments in his article on How to Embed Cultural Safety in Healthcare Governance – Better Boards. These developments include:
The Medical Board of Australia, public consultation on a draft revised code of conduct including a revised section on culturally safe and sensitive practice with Aboriginal and Torres Strait Islander peoples (June 2018).
The Nursing and Midwifery Board of Australia–care is ‘culturally safe and respectful’ (2018).
The Australian Health Practitioner Regulation Authority (AHPRA) committing to embedding cultural safety in the 15 national health practitioner boards (July 2018).
The Council of Australian Governments’ (COAG) Health Council public consultation on reforms of the Health Practitioner Regulation National Law (July 2018).
The National Safety and Quality Health Service Standards now contain six new actions for implementation in 2019, where achieving these actions means ‘provide culturally safe care’ for Aboriginal and Torres Strait Islander peoples (2019).
$350,000 for Australian-first online cultural safety training course for nurses and midwives delivering care to Aboriginal and Torres Strait Islander peoples (January 2019).
Recently, The Australian Health Practitioner Regulation Agency (AHPRA) asked for feedback on the definition of ‘cultural safety’ both from the public and specifically from Aboriginal and Torres Strait Islander individuals and organisations. The public consultation which closes next week (May 24th 2019) is led by the National Registration and Accreditation Scheme’s Aboriginal and Torres Strait Islander Health Strategy Group (Strategy Group) and the National Health Leadership Forum (NHLF), with the aim being to develop a definition that can be embedded more broadly. This is the proposed definition they want feedback on
‘Cultural safety is the individual and institutional knowledge, skills, attitudes and competencies needed to deliver optimal health care for Aboriginal and Torres Strait slander Peoples as determined by Aboriginal and Torres Strait Islander individuals, families and communities.
I really recommend reading the incisive and comprehensive critique of AHPRA’s definition of cultural safety in Croakey. Dr Leonie Cox (Queensland University of Technology) and Associate Professor Odette Best (University of Southern Queensland) argue that changing the definition from Māori scholar Dr Irihapeti Merenia Ramsden’s critical work replaces a political imperative with an individualised, ethnographic and idealised version which places the burden for health system transformation to the consumer in the guise of partnership. Cox and Best (2019) observe:
Let us be clear, cultural safety is about the cultures of systems, professions and practitioners. It is about an ongoing individual and organisational self-reflective exercise. It addresses the impact that mainstream cultures, ways of doing business and social positions have on practice and on health outcomes for service users.
I am pleased to have been involved in related initiatives happening in Victoria. In November 2018 I was invited to speak at the Victorian Clinical Council meeting, an independent group, which provides leadership and independent advice to the Department of Health and Human Services and Safer Care Victoria (SCV) on how to make the health system safer. The council had chosen the theme of diversity and cultural safety. In my presentation, I provided an overview of cultural safety. I also suggested a shift in focus from the language of diversity, to one that addresses power and privilege using critical tools like intersectionality and cultural safety. I shared the five facts about cultural safety and encouraged the council to ask disruptive questions and explore alternative ideas and perspectives. You can read more hereCommunique meeting 4 2018 (PDF, 130.27 KB). You can see the recommendations which will be presented to SCV and the department Secretary to endorse and action.
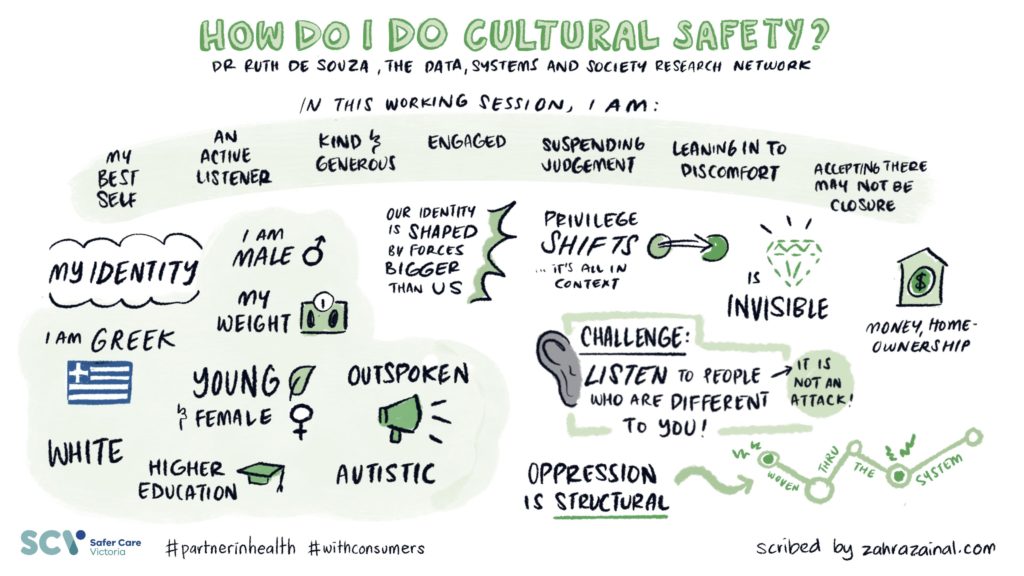
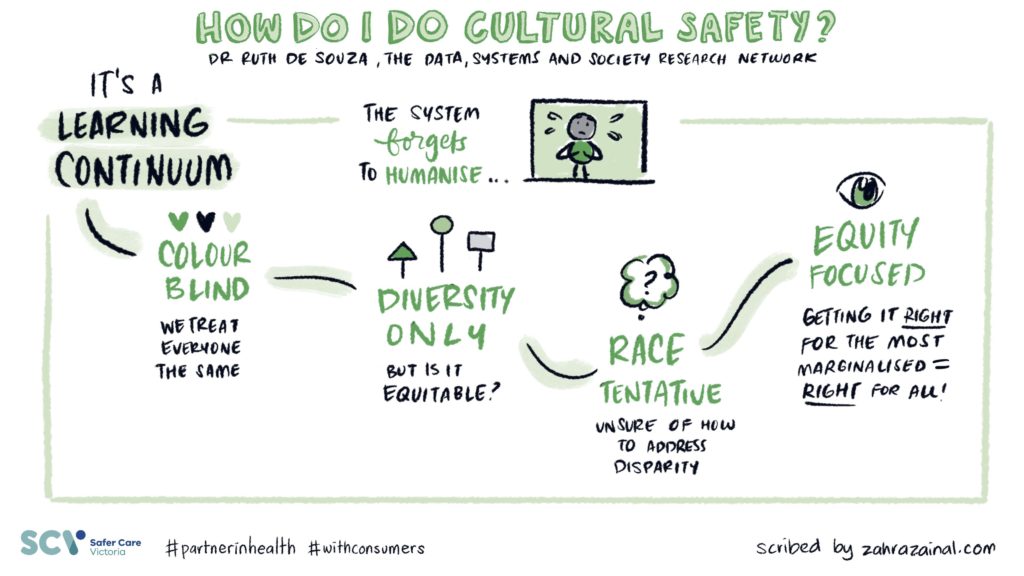
In April 2019, I was invited to be a keynote at Safer Care Victoria’s first Partnering in healthcare forum. The theme ‘Together is better’ is a reflection of a genuine commitment to ensure consumers are at the centre of care. Three hundred attendees attended the sold out event over two days to focus on how to best respond to the needs and expectations of consumers and deliver care that is person centred, equitable and caring. What impressed me ever so much is that Safer Care Victoria worked hard to support consumers to take part and over a hundred participants identified as having a consumer background. SCV have also developed a Partnering in healthcare framework. I have had a long interest in power relations in health and in examining how concepts like choice, partnership and empowerment can transfer responsibility to service users but without the access to infrastructure, resources and support. I loved David Gilbert’s presentation. David is a Consumer Director in the National Health Service, UK and he spoke about the role of consumers and patients and how the notion of ‘patient leadership’ in the UK is transforming roles, opportunities, and models of patient partnership. In a fabulous article in the BMJ, David says:
Meanwhile, I watch the failure of the engagement industry—reliant on child-parent feedback mechanisms and adolescent-parent institutional arrangements that pit representatives against professionals (or co-opt them) in tedious sub-sub-committees. And yields… not much to be honest. Everywhere I look, power is neutralised and buffered. We are patted on the head, told to play with broken toys rather than join in with the big boys. The passion and wisdom gained through suffering and resilience is not valued. This is a caricature, but I believe it largely represents recent reality.
I really appreciated what David said about what we call people who try to change the system rather than healing in peace. occupy what do we call idiots like me who, instead of just wanting to heal in peace, return to the NHS in a different guise?
There were so many other highlights at the Partnering Forum which gave me great heart. One of the standouts (and I know I should mention every single one) was by Clinical Lead and Facilitator for the Rounds, Associate Professor Leeroy William, Chief Experience Officer Anne Marie Hadley and Anjali Dhulia from the Schwartz Round team who provide palliative care at Monash Health. This team were highly commended in the Safer Care Victoria compassionate care award category for the ‘Rounds’ which are a structured forum for all clinical and non-clinical staff. It provides a safe and nurturing space for people to regularly come together to talk about the emotional and psychological aspects of working in health care. The idea comes from work at the Schwartz Centre for Compassionate Care in Boston. What I loved about it, is the recognition of trauma and compassion fatigue for people who work in health care which includes staff like cleaners or kitchen staff who do not get seen as part of the health care team, but often have very intimate conversations and connections with people. I think that having the space to talk about things that matter in the factory system of health care can transform burnout, negativity and cynicism, by providing a sense of community and care and mostly reconnecting people to their purpose in working in health.
Which brings me to my own presentations at the conference. I did a keynote presentation and a workshop. Rather than attempt to summarise, I’ll leave the last words and images to the most fabulous Zahra Zainal, a Melbourne-based graphic recorder and illustrator, who has so much talent and was able to simplify and amplify my words into stunning illustrations. Please feel share to use and share with appropriate acknowledgement of Zahra and I.
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2019/05/07_EquityInclusionInHealthcare.original.1556573312-1024x576-1.jpg5761024ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2019-05-20 14:12:232019-05-20 14:12:23Cultural safety: On healing the health system through partnership
I wrote a piece for the Spring 2018 edition (Issue 23) of the Hive (the Australian College of Nursing’s quarterly publication). Cite as:DeSouza, R. (2018). Is it enough? :Why we need more than diversity in nursing. The Hive (23, 14-15). You can also download a pdf of the article for your own personal use.
Diversity is a hopeful, positive and celebratory idea, it generates more happiness than words like inequity, racism and privilege. It feels good for a large number of people precisely because it is depoliticized (Hall & Fields, 2013). It does not demand accountability. It does not demand transformational change of our minds or our environment, but requests that we continue to put up with difference or to tolerate it (Bell & Hartmann, 2007). What does it mean for our profession to be diverse? And is it enough?
Is it enough, when we have a yawning chasm of health inequity and disparity, of deaths in custody, of punitive policy aimed at Aboriginal Australians? Is it enough, in an era of devastating Islamophobia and racism enabled by nationalist right wing xenophobia? Is it enough, when politicians challenge group-based rights and argue that they undermine social cohesion and “our way of life”, maligning and scapegoating already vulnerable groups like African youth. Is it enough, when media only catapult the spectacular and exceptional into our view. Is it enough, when the entire world is condemning Australia’s abhorrent offshore policy of deterrence and detention. Yes, we need to recognise difference, but we must also understand how differences are connected to inequalities. As Mohanty observes: “diversity by passes power as well as history to suggest a harmonious and empty pluralism” (Mohanty, 2003, p. 193).
We might be ticking the diversity boxes and celebrating diversity — whether in University brochures and websites or on Harmony Day — but do our combined activities address health disparities? The problems of inequity and disparity are bigger than us but we can be accountable for the parts we play in larger political struggles. For a politics of equity, we also need to consider race, disability, ethnicity, class, gender, sexuality, and religion and integrate these into our analyses of our social world. We need to expand the frames we use to look beyond individual behaviour and to consider social and systemic issues, and call for systematic interventions to address inequity. ‘Celebrating’ cultural difference isn’t the same as action, as fighting for justice. As (Perron, 2013) notes, nurses can be both caring for individuals and advocating for the collective rights to equitable care, they aren’t mutually exclusive.
Diversity assumes that care is still a neutral technical activity
As nursing emerged from being a class of handmaidens to the medical system to the dynamic profession it is today, we have understood it to become an intellectual, cultural and contextual activity. This means it is also a political activity (De Souza, 2014). Nursing is connected to systems of power and privilege. Nurses and clients bring multiple ways of being in the world into the world of care and yet we only privilege some of these ways of being. Iris Marion Young describes oppression as being “the disadvantage and injustice some people suffer not because of a tyrannical power coerces them but because of the everyday practices of a well-intentioned liberal society…” (Young, 1990, p. 41). There continue to be clear links between institutional bias in health care systems and health disparities (Hall & Fields, 2013). Let’s ask ourselves what practices we enact every day that contribute to inequity?
Diversity maintains whiteness at its core
In diversity talk in nursing there’s an assumed white centre with difference added. White people are conceived as the hosts and people of color viewed as guests and the perspectives of Indigenous people are erased. Allen (2006, pp. 1–2) calls this the ‘white supremacy’ of nursing education: an assimilationist agenda that converts diverse groups people into a singular kind of nurse, which can then add ‘others’ into the mainstream to create a multicultural environment. But, this addition reinforces rather than displaces whiteness from the centre of structures and processes of educational or clinical institutions (p.66). It’s important that we focus on whether nurses reflect the communities that they serve. But representation in the workforce doesn’t mean that the people who are culturally different have a voice in the corridors of power. There are questions also about “who’s at the decision-making table and who’s not. And what’s on the agenda and what’s not” (Brian Raymond, 2016).
Diversity focuses on sensitivity and respect rather than on the social and historical
Race and racism are determinants of health inequities (Krieger, 2014) therefore it follows that a key area where nurses could intervene is to address discrimination. It is inadequate for us to provide individualised sensitive and respectful care while ignoring the historical and structural conditions that shape health and healthcare. As nurses, we understand more than most that life is an uneven playing field – we need to bring this knowledge to the way we work as a profession. Cultural sensitivity and awareness tend to assume that racism is “out there”, rather than something that is also enacted within healthcare systems. Our claims to colorblindness reinforce the problem, as” treating people the same” doesn’t take into account their differing needs, which is one definition of what care is.
Spotted at my local market
Creating a meaningful diverse and multicultural nursing profession
in an era where both patient populations and the nursing workforce are becoming more diverse, where are the spaces for nurses to talk about both institutional and societal racism and how they impact on care? How can nurses broaden their focus from the micro-level to see the big picture, especially when they labor in unstable and under-resourced working environments (Allan, 2017)? Nurse educators must confront our own resistance to teaching about race and racism (Bond & Others, 2017) – the recent debates about the inclusion of cultural safety into the Nursing and Midwifery Codes of Conduct reflect now far we have to go. Our curricula must more explicitly embed anticolonial and intersectional perspectives into learning experiences in order to prepare nurses for not only understanding how structural inequities affect health but also for the skills to counter them (Blanchet Garneau, Browne, & Varcoe, 2016; Thorne, 2017; Varcoe, Browne, & Cender, 2014). In Australia, the Indigenous Health Curriculum Framework developed by the Committee of Deans of Australian Medical Schools, recognised the critical need to teach students about racism. In particular, it asks us to see the connection between history and current health outcomes; to be able to identify features of overt, subtle and structural racism or discrimination and to be able to address and help resolve these occurrences.
Viewing nursing as a neutral, universal activity where appreciation, sensitivity and respect are adequate, prevents us from considering nursing as a political activity where power is at play. Conversely, embedding an understanding of the historical, structural and systemic factors that shape health, into our practice will allow us to create a meaningfully inclusive – and more caring – profession. This however, requires courage, commitment and accountability. Do we have it?
References
Allan, H. (2017). Editorial: Ethnocentrism and racism in nursing: reflections on the Brexit vote. Journal of Clinical Nursing, 26(9-10), 1149–1151.
Allen, D. G. (2006). Whiteness and difference in nursing. Nursing Philosophy: An International Journal for Healthcare Professionals, 7(2), 65–78.
Bell, J. M., & Hartmann, D. (2007). Diversity in Everyday Discourse: The Cultural Ambiguities and Consequences of “Happy Talk.” American Sociological Review, 72(6), 895–914.
Blanchet Garneau, A., Browne, A. J., & Varcoe, C. (2016). Integrating social justice in health care curriculum: Drawing on antiracist approaches toward a critical antidiscriminatory pedagogy for nursing. Sydney: International Critical Perspectives in Nursing and Healthcare. Google Scholar. Retrieved from http://sydney.edu.au/nursing/pdfs/critical-perspectives/blanchet-garneau-browne-varcoe-integrating-social-justice-2.pdf
Bond, C., & Others. (2017). Race and racism: Keynote presentation: Race is real and so is racism-making the case for teaching race in indigenous health curriculum. LIME Good Practice Case Studies Volume 4, 5.
Brian Raymond, M. P. H. (2016, August 2). How Racism Makes People Sick: A Conversation with Camara Phyllis Jones, MD, MPH, PhD | Kaiser Permanente Institute for Health Policy. Retrieved August 17, 2018, from https://www.kpihp.org/how-racism-makes-people-sick-a-conversation-with-camara-phyllis-jones-md-mph-phd/
De Souza, R. (2014). What does it mean to be political? Retrieved August 21, 2018, from http://ruthdesouza.dreamhosters.com/2014/08/03/what-does-it-mean-to-be-political/
Hall, J. M., & Fields, B. (2013). Continuing the conversation in nursing on race and racism. Nursing Outlook, 61(3), 164–173.
Krieger, N. (2014). Discrimination and health inequities. International Journal of Health Services: Planning, Administration, Evaluation, 44(4), 643–710.
Mohanty, C. T. (2003). “Under Western Eyes” Revisited: Feminist Solidarity through Anticapitalist Struggles. Signs: Journal of Women in Culture and Society, 28(2), 499–535.
Perron, A. (2013). Nursing as “disobedient” practice: care of the nurse’s self, parrhesia, and the dismantling of a baseless paradox. Nursing Philosophy: An International Journal for Healthcare Professionals, 14(3), 154–167.
Thorne, S. (2017). Isn’t it high time we talked openly about racism? Nursing Inquiry, 24(4). https://doi.org/10.1111/nin.12219
Varcoe, C., Browne, A., & Cender, L. (2014). Promoting social justice and equity by practicing nursing to address structural inequities and structural violence. Philosophies and Practices of Emancipatory Nursing: Social Justice as Praxis, Eds PN Kagan, MC Smith and PL Chinn, 266–285.
Young, I. M. (1990). Throwing Like a Girl and Other Essays in Feminist Philosophy and Social Theory. Monograph Collection (Matt – Pseudo).
https://ruthdesouza.dreamhosters.com/wp-content/uploads/2018/11/Embracing-diversity-scaled-1.jpg22722560ruthhttp://ruthdesouzastage.local/wp-content/uploads/2024/12/spa_logo-300x138.pngruth2018-11-14 20:53:132018-11-14 20:53:13We need more than diversity in nursing.